KLAS Report Deciphers Speech-Recognition Trends
Informatics Report: Top 10 Reasons PACS Projects Fail or Fall Short
Big Deal
Running the Numbers
FDA Approved: Enterprise Solution Receives 510(k) FDA Clearance
FDA Approved: Kodak?s New PACS Capabilities Earn FDA Clearance
Product Showcase: Mediplus Releases Inexpensive DICOM Modality Worklist Server
KLAS Report Deciphers Speech-Recognition Trends
by Dana Hinesly
The use of back-end speech recognition (SR) is growing, according to a recent report from KLAS Enterprises LLC (Orem, Utah) that details the sentiments and trends among professionals using the technology. Back-end systems allow physicians to dictate reports and then forward the text and audio files to a third party for polishing. However, they typically don’t provide the savings found with front-end SR systems, which require the user to read, edit, and complete the report in one sitting.
“The impact to the physicians themselves is materially less, because in the back-end solution, it’s very rare that users are going to edit the reports themselves,” said Jeremy Bikman, director of imaging and advanced technology at KLAS, a research and consulting firm specializing in monitoring and reporting on the performance of health care information technology (HIT) vendors and professional services firms. “With back-end speech recognition, you minimize the impact on the clinician—who can speak into a microphone and be done—so is it an easy thing for him or her to do.”
 |
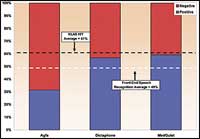
| Figure 1. Front-end SR vendors score an average 49% in positive vs negative commentary average, significantly below the KLAS HIT positive commentary average (all vendors, all products in the KLAS database) of 61%. (Click image for larger view) |
This year’s report also saw SR beginning to emerge in departments beyond radiology, including pathology, cardiology, and internal medicine. The back-end offerings are expanding in all areas of acute care and ambulatory care delivery.
Edging Toward Perfection
SR technology is improving, but there is still considerable room for improvement, according to the feedback KLAS received. The wish list for the types of enhancements respondents are interested in seeing includes “more robust speech recognition in general, including improved handling of foreign speakers, regional accents, and filtering of background noise,” alongside hopes that future versions will integrate more readily with other software applications. Other areas of possible development are the inclusion of practical ways to resume interrupted dictations and better management reporting.
Benefits were found in both forms of SR systems, regardless of whether front- or back-end implementation was used. According to the report, “The largest quantifiable benefits reported were turnaround time on the front-end systems and increased productivity and turnaround time on the back-end systems.” (Figures 1 and 2)
 |
| Figure 2. Back-end SR vendors (75%) score above the KLAS HIT positive commentary average (all vendors, all products in the KLAS database) of 61%. This is a very good percentage rating, particularly in contrast with the front-end percentage of 49%. (Click image for larger view) |
When systems perform as intended, savings also are realized in both front- and back-end modes. In situations where the recognition rate is very high and clinician acceptance and usage is high, front-end systems can achieve significant savings. When recognition isn’t substantial, there is significant frustration and a marginal level of financial gain.
Savings are found in back-end implementations primarily due to the fact that transcriptionists are not creating documents from scratch; rather, they are simply editing with the assistance of software. The use of templates and tools also can speed dictation time.
“We’re seeing a lot of growth with the transcriptionist or outsourced transcription vendors using back-end speech,” Bikman said. “There continues to be an emerging trend of the providers themselves requiring, or strongly suggesting, to their outsourced transcription vendor that they use a back-end speech solution.”
Study Details
The study included 13 vendors and 14 products, focusing on front- and back-end SR software products and vendors for health care providers. Only vendors with a minimum of 15 unique acute care organizations reporting were included in the “main body” of the study.
Scores (out of 100) for the front-end vendors in this category were:
- 85.9 for SpeechQ from MedQuist Inc (Mount Laurel, NJ);
- 79.9 for PowerScribe from Dictaphone, now part of Nuance Communications Inc (Burlington, Mass); and
- 62.7 for TalkStation from Agfa Corp (Ridgefield Park, NJ).
Back-end main body ratings scores (out of 100) were:
- 91.4 for EditScript from eScription Inc (Needham, Mass); and
- 75 for EXSpeech from Dictaphone.
The average performance score for SR vendors in the KLAS Database is 79.5, with front-end main body vendors ranging between 62.7 to 85.9 and back-end main body vendors ranging from 75.3 to 91.4.
Note: The data and charts used in the compilation of this story are from the “2006 Speech Recognition Report,” published in April 2006, and have been reprinted with permission from KLAS. Visit www.healthcomputing.com for more information. The report and all of its data is KLAS Confidential Information. ? 2006 KLAS Enterprises LLC. All rights reserved.
Informatics Report: Top 10 Reasons PACS Projects Fail or Fall Short
More times than not, I encounter people who tell me that they had pursued their PACS project only to have it fall apart at some stage—and they are at a loss to understand why. Here, for those who are struggling with their PACS projects, I give you my top 10 reasons why PACS projects don’t meet expectations.
1) Poor Planning. Many times, projects seem to have no overall time line with key activities locked down. The only timing that appears to be the driving milestone is budget-related—an estimate of what can be done with the given budget is thrown together to see what sticks. The result is a project half done and poorly built with blame being pointed all around. Solution: Plan ahead!
 |
2) Vendor Teaching. Say you have a vendor with whom you have worked for many, many years. The vendor is a trusted advisor and has a strong salesperson. Independent of its PACS offering, the vendor brings in its own “specialist” to tell you exactly what you need to buy. Of course, the number magically totals to the exact amount you have budgeted (and shared with them). When the vendor “advises” you on what to buy, is that educating or selling? How do you really know what you are—or aren’t—getting? Solution: Every project has several options for building a system; know your options.
3) Poor Teaming. Successful projects are a by-product of key stakeholders working together. They communicate openly and honestly about which product will be the best fit for their team. They also disclose what the trade-offs would be to select a different vendor. In many cases, certain team members become adamant about what they want and are unwavering in their demands, which results in failure. Solution: Involve the right people who understand the art of compromise.
4) Politics. Anytime politics are the overriding factor in vendor selection, the project is doomed. We know that some level of politics is typically involved, but if it’s mandated from on high that you must buy from vendor X, you are being set up for failure. Solution: Carry out proper political due diligence to help you prepare.
5) Incomplete System Design. The PACS solution itself is only half of what you need and does not include other key pieces. I have witnessed sites that have hooked up a couple of modalities and sent the images to an archive, and the staff members believe it’s a good first step in a 2- or 3-year plan. If you want to spend money and guarantee no return, you will be absolutely correct. Solution: Know your true needs for building and using a complete system.
6) Focus on Money. Money is always an issue ? always, always, always. In fact, several reasons for failure on this list can be attached by dotted line to money. Not having enough money, time constraints on the availability of money, or the lack of other strategic plans for the funds will force you to either buy something that is of low value or does not allocate your dollars for the biggest return. Solution: Again, know your true needs and then budget accordingly.
7) Incomplete Budget. You are almost better off to buy nothing than to buy bits and pieces that add work for an organization but deliver little to no benefit. Hospitals are doing this every day. Solution: Don’t kid yourself—the saying “you get what you pay for” certainly applies to PACS.
8) Incorrect Trade-offs. If you must make any project trade-offs to bring the project to budgeted levels, what can be done? Shortcuts will deliver exactly that—an incorrect trade-off. And unless you are very lucky, you are destined to underachieve. Solution: Determine the true effect of each trade-off.
9) Lack of Facility Readiness. What needs to be done, and who needs to do it? These usually are facility-generated delays, because your PACS vendor doesn’t do everything. Solution: Make a list of items that need to be planned for and completed well in advance of delivery of any vendor hardware or software. Note: The list will be long.
10) Failure to Know What You Don’t Know. Typically, this problem ends up being an issue of one or two people going to a couple of trade shows, listening to several vendors, listening to a few speakers, reading some articles, or joining some online chats. Many times, advice is given by someone who has a data point of 1. Solution: Know how much weight to put on the provider of your information.
Michael Mack is VP of business development at the Thomas Group Ltd (Anaheim, Calif). Having more than 20 years of experience in the medical-imaging industry, Mack now specializes in PACS planning and implementation.
Big Deal
- Proscan Imaging Inc (Cincinnati) recently installed the IntelePACS system from Intelerad Medical Systems (Montreal) at its centers across the United States. Proscan, a large teleradiology service provider, has facilities in 43 states and specializes in MRI interpretation. The company boasts attending radiologists in a number of subspecialties, including musculoskeletal, neurology, cardiac, and breast imaging. Proscan chose the IntelePACS system for its efficacy at handling of high image volume—a crucial feature for minimizing diagnostic time, and one that will only become more valuable as Proscan grows.
- The Grey Bruce Imaging Network (Owen Sound, Ontario) has selected the Carestream PACS and Enterprise Information Management system from Eastman Kodak Co (Rochester, NY) to handle its 11-hospital regional network. The system will be housed on Grey Bruce’s network that manages 175,000 imaging studies annually. The Carestream PACS will be combined with a RIS from Cerner Corp (Kansas City, Mo), the Powerscribe speech-recognition system from Dictaphone (now a part of Nuance Communications Inc of Burling-ton, Mass), and built-in access to orthopedic surgical templates from OrthoView (Hampshire, UK).
Running the Numbers
$73.6 million is the earned revenue of the European cardiology PACS market in 2005, according to Frost & Sullivan (London). The global growth consulting company estimates revenue to reach $200.5 million in 2012. For more information, visit www.medicalimaging.frost.com.
FDA Approved: Enterprise Solution Receives 510(k) FDA Clearance
 |
| Now FDA cleared, Voxar 3D Enterprise incorporates off-the-shelf server and graphics cards technologies so that users benefit from the latest computer technology advances. |
Barco (Duluth, Ga) has received 510(k) pre-market approval from the FDA for its enterprise solution that delivers rapid access to advanced visualization analysis. Voxar 3D Enterprise accelerates the speed at which technologists, radiologists, and physicians can load, review, report, and communicate large volumetric image studies throughout the enterprise. Using high-performance graphics cards, Voxar 3D Enterprise provides quick access to Voxar 3D’s advanced visualization tools—both inside and outside the radiology reading room. Voxar 3D enterprise can be integrated directly into an existing PACS; it also can be directly integrated into the radiology workflow where PACS is not present.
FDA Approved: Kodak?s New PACS Capabilities Earn FDA Clearance
 |
| The newest version of Kodak?s Carestream PACS software equips radiologists with integrated cardiac review and analysis, cardiac cage removal in 3D imaging, and cardiac calcium scoring functionality while reviewing cardiac CT exams. |
Eastman Kodak Co (Rochester, NY) has received clearance from the FDA for several specialized functions that enable radiologists to better diagnose from images generated by noninvasive cardiac scanning methods on the vendor’s PACS workstation. These specialized functions—cardiac review and analysis, cardiac cage removal in 3D imaging, and cardiac calcium scoring—are being integrated into the latest version of the Carestream PACS software. The functions equip radiologists to analyze cardiac CT imaging exams and will be commercially available in the newest version of Kodak PACS software, scheduled for release mid-2006.
Cardiac review and analysis provides four-chamber and cross-sectional views of the heart axis as well as panoramic and cross-sectional views of cardiac vessels. The calcium scoring module analyzes calcified plaque in five main blood vessels of the heart, and the cage removal function removes anatomy around the heart not required for cardiac viewing.
The company also received FDA clearance for a bone-removal feature (to enhance viewing of other structures) and vessel analysis enhancement (including extended stenosis marking).
Product Showcase: Mediplus Releases Inexpensive DICOM Modality Worklist Server
 |
| Fast Worklist from Mediplus Software is available in five languages?English, French, Italian, Portuguese, and Spanish. Soon, it will support Polish. |
Mediplus Software (Sao Paolo, Brazil) has released Fast Worklist, a DICOM modality worklist server that can be used in a variety of settings, from physicians’ offices to mid-sized facilities with one or more modalities. The server automatically retrieves patient and study information from any available modality, eliminating the need to reenter data at the source and avoids errors. Additionally, it improves overall productivity and guarantees study data is catalogued correctly. Fast Worklist allows operators at each modality to retrieve a list of scheduled studies to perform and automatically enter the correct patient information.

