|
· TomoTherapy Brings IMRT, IGRT to Wisconsin Clinic
· Combination Therapy Shows Promising Results
· FDG-PET Findings Influence Clinicians? Decisions
TomoTherapy Brings IMRT, IGRT to Wisconsin Clinic

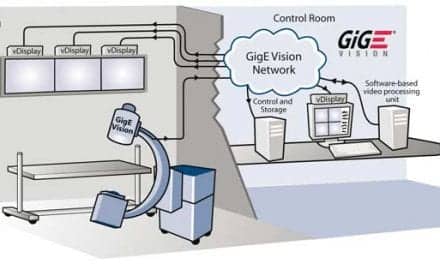
When James S. Welsh, MS, MD, initially arrived at the University of Wisconsin, he had been specifically recruited to conduct scientific evaluations of helical tomotherapy. His research found that the unit produced megavoltage CT images that allowed for image-guided radiation therapy, in addition to delivering intensity-modulated radiation therapy.
“Our initial dosimetric investigations hinted that this technology had the potential to match or exceed even the most exquisite dose distributions previously achievable with conventional linac 3D conformal radiotherapy or other IMRT approaches,” said Welsh, one of the first physicians to treat human patients with the new technology.
In the meantime, TomoTherapy Inc, Madison, Wis, was perfecting its TomoTherapy Hi-Art treatment system, a radiation therapy device with a built-in CT scanner that was designed to provide IMRT, IGRT, and adaptive therapy.
 |
| The TomoTherapy Hi-Art treatment system provides IMRT, IGRT, and adaptive therapy for a wide range of cases. |
After Welsh was invited to present his research at various conferences and international meetings, his patients at a small outreach facility in which he also worked began to ask him if they would be receiving the innovative treatment. Welsh, medical director at University of Wisconsin Cancer Center-Riverview in Wisconsin Rapids, said he would feel badly informing his patients that TomoTherapy was not available for them at the clinic. However, “Riverview Hospital then ventured out on a limb and became the first small community hospital to have a TomoTherapy-only clinic with remote dosimetry,” Welsh said, explaining that his dosimetrists were stationed in Wausau, a city 50 miles away.
TomoTherapy CEO Fred Robertson said the future of radiation therapy is incumbent upon the clinician’s ability to utilize image guidance and adapt the plan on a daily basis. Through the CT scanner, clinicians can image patients daily before each treatment, and then they can use the 3D images to determine whether treatment plan margins are still on target. Robertson said the ring gantry geometry makes it possible for 360? IMRT delivery utilizing a highly conformal treatment dose. With the system’s fully integrated Planned Adaptive software, true adaptive radiation therapy can be offered. This software helps in the evaluation of dose and the application of changes to the treatment plan.
The highly conformal treatments spare normal tissue and hit targets tightly with intended doses, Robertson said. The process is completely integrated, from treatment planning to quality assurance, patient setup, and treatment delivery. “The TomoTherapy Hi-Art treatment system allows clinicians to treat a wide range of cases from head and neck, to breast, to prostate, to total body irradiation,” Robertson said. “Whether the case is simple or complex, the quality of a TomoTherapy treatment remains the same. Often, our competitors stumble upon this because with increasing treatment plan complexity often comes decreased quality.”
TomoTherapy creates dose distributions that are inherently less likely to cause long-term toxicity than older methods, said Welsh, also clinical associate professor of human oncology and medical physics at the University of Wisconsin. With TomoTherapy, radiobiology advances can make way for improved cure rates through larger daily doses over a shorter period of time, he continued.
One of the most exciting and rewarding new applications of the technology, according to Welsh, allows for stereotactic body radiation therapy, which involves the administration of very large doses over a short period of time to tumors in the lung, liver, spine, or other extracranial sites. Welsh said he was surprised by how many patients who are diagnosed with Stage I lung cancer cannot have surgery for medical reasons.
“This is a far easier treatment for most patients compared to thoracotomy and may offer a curative option for those who are not suitable surgical candidates,” said Welsh, who is also investigating the treatment’s benefits for breast cancer patients. “This is now routinely available here in the community, and I believe it has proved beneficial to many early-stage lung cancer patients who otherwise had no hope.”
Expensive cost comes with the reality of offering the most sophisticated treatment available, Welsh points out. It also requires significantly more time, thought, and effort on the part of the physicians, dosimetrists, and physicists involved, he said.
“However, the technical reimbursements are presently favorable, and most importantly, the treatments hold promise for improved outcomes for our patients,” Welsh said. “I think anyone would agree that a little more time and effort is certainly worth it if patient outcomes can be improved. And it does look like that is possible now.”
Combination Therapy Shows Promising Results
With 32,000 people dying of pancreatic cancer each year, the disease is the fourth-leading cause of cancer death in the United States. Only 4% of people are still alive 5 years after they were diagnosed.
Surgery is the treatment of choice for these patients, but less than 14% of them are eligible because the disease is usually diagnosed at an advanced stage.
Nevertheless, a new study conducted by the Radiation Therapy Oncology Groups has revealed some promising news—the addition of gemcitabine to standard chemoradiotherapy following surgery improved survival for patients with the most common form of pancreatic cancer.
A clinical research component of the American College of Radiology, the RTOG and its investigators found that the new, well-tolerated therapy was associated with a demonstrated survival benefit. Yet, because the improvement was not statistically significant, researchers determined that more effective systematic therapies are still needed to prevent recurrence of the often-fatal disease.
The study, called RTOG 9704, was part of a 4-year, multicenter trial that was the largest clinical study of its kind and the first phase III clinical trial in the United States in 3 decades to look at adjuvant treatment for pancreatic surgery patients. Funded by the National Cancer Institute, part of the National Institutes of Health, the trial focused on patients with pancreatic head adenocarcinoma, or cancer of the head of the pancreas. Results were published in the March 5 issue of the Journal of the American Medical Association.
“This study will change standard practice across the country for postoperative treatment of this type of pancreatic cancer,” said William F. Regine, MD, principal investigator, professor and chairman of radiation oncology at the University of Maryland School of Medicine, and chief of radiation oncology at the University of Maryland Marlene Stewart Greenebaum Cancer Center. “Although the results are not considered statistically significant, they are clinically meaningful. There was consistent improvement in survival among patients with cancers of the head of the pancreas that received gemcitabine, at least up to 3 years following diagnosis.”
According to Walter J. Curran, Jr, MD, RTOG group chair, the Lawrence W. Davis professor and chair of the Department of Radiation Oncology in the Emory School of Medicine, and the chief medical officer of the Emory Winship Cancer Institute, the RTOG has reported the preliminary results of the study at major cancer society meetings. Many oncologists are already using the new combination therapy with gemcitabine to treat patients postsurgery, he added.
Gemcitabine, an antimetabolite that interferes with the growth of cancer cells, is used to treat patients with advanced pancreatic cancer who are not eligible for surgery, as well as other cancers. The randomized controlled phase III trial included 451 eligible and analyzable patients enrolled between July 1998 and July 2002 at 164 institutions throughout the United States and Canada, with follow-ups through August 2006.
Thirty-one percent of the participants with pancreatic head adenocarcinoma were still alive 3 years after diagnosis following surgery and treatment with gemcitabine, chemotherapy drug 5-fluorouracil, and radiation. Those who were treated with 5-FU and radiation alone—the standard postoperative treatment for this type of cancer since the 1980s—showed a 22% 3-year survival rate.
The median survival rate for patients who received gemcitabine was 20.5 months, versus 16.9 months for patients who received the standard treatment. Researchers did not see any benefit of adding gemcitabine for patients with cancer in other parts of the pancreas.
Regine said the study’s patients had the lowest rate of cancer recurring in its original location than in any previous study. The tumor came back in the same area in 23% of the patients, compared to 40% to 60% of patients in other studies. However, 70% of the patients in this study experienced metastasis.
“Clearly, metastatic disease is a huge problem, and we need more clinical research to identify new systemic or targeted therapies to prevent this type of recurrence,” Regine said.
RTOG researchers are in the planning stages of testing new agents, using the new combination therapy of gemcitabine, 5-FU, and radiation as the standard. They also will examine the genetic profiles of the cancers to help determine patients’ responses to a particular therapy, which would allow physicians to tailor treatments to individual patients.
In addition to the RTOG, two other NCI-funded cooperative groups—the Eastern Cooperative Oncology Group and the Southwest Oncology Group—were involved in the study.
FDG-PET Findings Influence Clinicians’ Decisions
FDG-PET scan findings influenced clinicians’ methods of care for more than one in three cancer patients, according to a study published in the March 24 edition of the Journal of Clinical Oncology.
Data from the National Oncology PET Registry, launched in May 2006 by the Centers for Medicare and Medicaid Services, revealed that the scans are associated with a 36.5% change in the decision of whether, or how to, treat a patient’s cancer.
Information from nearly 23,000 patients representing more than 1,200 facilities nationwide contributed to the NOPR study. “The NOPR working group sought to measure the impact of PET findings on patient management in a manner minimally intrusive to care providers,” said study author Bruce Hillner, MD, professor and eminent university scholar in the Department of Internal Medicine at Virginia Commonwealth University. “This was critical for successfully collecting the large amount of data required for a robust analysis.”
Launched in response to CMS’ “Coverage with Evidence Development” policy, the NOPR collects data to inform the center’s FDG-PET coverage determination decisions for currently noncovered cancer indications. The group is sponsored by the Academy of Molecular Imaging and managed by American College of Radiology and the ACR Imaging Network.
Regarding the study’s findings, NOPR working group co-chair R. Edward Coleman, MD, said, “We were especially surprised by the impact of the PET findings on patients who were originally planned to have a biopsy.”
“The procedure was avoided in approximately three-quarters of these patients,” continued Coleman, a professor of radiology and chief of the Division of Nuclear Medicine at Duke University School of Medicine.
Anthony Shields, MD, who also serves as NOPR working group co-chair, said the results confirm what oncologists suspected from their increasing experience with PET.
“However, we lacked the significant data required to prove the benefit of PET for many uncovered indications,” said Shields, professor of medicine and oncology at the Karmanos Cancer Institute at Wayne State University. “It’s very encouraging that oncologists and other clinicians may have access to the valuable information PET affords for ensuring the best patient care.”
Medicare’s reimbursement coverage includes cancers of the ovary, uterus, prostate, pancreas, stomach, kidney, and bladder.