A recent survey points to increased interest in comparative effectiveness research. Experts say radiology should be prepared to demonstrate the value of imaging with CER data.
The rising cost for health care represents a massive challenge for public and private payors, and both have looked for transparent opportunities to constrain costs without compromising on quality. In addition, concerns that health care decision-makers do not have the information needed to make the best decisions about how to diagnose or treat medical conditions have led to the emergence of comparative effectiveness research (CER). As described by the Institute of Medicine in a 2009 Consensus Report, the purpose of CER is to assist consumers, clinicians, purchasers, and policy makers to make informed decisions that will improve health care at both the individual and population levels.1
In an effort to provide information about the best available evidence to help patients and their health care providers make more informed decisions, the Patient-Centered Outcomes Research Institute (PCORI) was established by Congress through the 2010 Patient Protection and Affordable Care Act.2 However, it is by law an independent, nonprofit organization. The goal of PCORI is to produce information patients and their health care providers can trust. The results of PCORI’s research are to be provided to patients and clinicians in ways that are responsive to their needs and interests and easy to understand. PCORI is an information resource, not a care provider, and will ensure that its research is not construed as mandates for practice guidelines or coverage recommendations.
In general terms, efforts to assess the effectiveness of different treatment options can be pursued in a variety of ways. The methods range from synthesizing existing research—a process known as a systematic review—to funding new head-to-head clinical trials. The level of evidence needed and the level of sophistication to support that evidence as well as the balance between pros and cons of each method evidently dictate how data are generated. In an ideal world where time and money were not an issue, head-to-head clinical trials done in different settings (academia vs community) would be preferred as they most often provide the highest level of evidence. But in today’s cost-containment environment, creative ways have to be employed to minimize barriers.
As diagnostic imaging represents a notable and often targeted portion of health care costs, more scrutiny has been placed on CER and how it could specifically be applied to radiology. In an article published in Radiology in 2009, Pandharipande and Gazelle3 highlighted the need to develop a strong CER infrastructure for radiology. Unique challenges and barriers to applying CER to radiology include rapidly changing technology, complex care processes, and the difficulty of demonstrating the true impact of a diagnostic exam on patient outcomes.4
Unlike pharmaceutical intervention, which is therapeutic in nature, there is often a gap between diagnostic imaging and outcomes. Even though several studies have shown a link between them (eg, association between imaging services during an admission and lower mortality and shorter length of stay for patients receiving imaging earlier in their admissions), the direct linkage to patient outcomes for imaging remains a challenge. Diagnostic tests have immediate outcomes: they will influence the treatment course when done in a timely manner and appropriately but will not in general directly affect patients’ health outcomes. Imaging’s rapidly evolving technology adds to the difficulty of applying CER to radiology as technologies studied in large trials could become obsolete by the time the results were available. Finally, imaging is sometimes just one step in a complex process and one component of a multitude of actions, from the physician ordering the test to the radiologist interpreting the image. One can easily imagine the challenges of demonstrating the specific benefits of a test and discriminate them from the other steps of a multistep process and other variables (such as timing and setting) that can have an impact on outcomes.
Despite these challenges, results from a survey aimed at observing physicians’ perceptions in regard to comparative effectiveness research show an increased support between 2009 and 2011.
Methodology
Office-based physicians (358 in 2009 and 359 in 2011) were surveyed online by Harris Interactive. The respondents included 70% primary care and 30% specialists. The first sample was surveyed in the fourth quarter of 2009 and the second in the first quarter of 2011. One of the poll questions sought to determine attitude toward CER among office-based physicians. The following 5-point Likert scale was used to assess physicians’ support for CER: strongly support, somewhat support, neither support nor oppose, somewhat oppose, and strongly oppose. Another question aimed at evaluating the likelihood for physicians to implement CER in five different situations: (1) recommendations for surgical procedures, (2) prescribing decisions, (3) recommendations for diagnostic imaging, (4) recommendations for preventive care, and (5) shared decision-making with patients. Similar to the other question, a 5-point Likert scale was used with answers ranging from extremely likely to not at all likely. The study was an independent poll, which was not financed by industry interests.
Findings

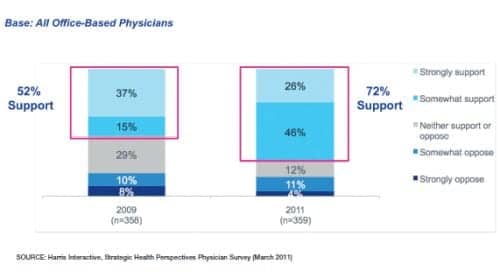
Figure 1: Increase in CER support among Physicians

Figure 2: Physicians most likely to implement CER in their shared decision-making and preventative care recommendations, but more than half say they will implement in diagnostic imaging and prescribing decisions.
The results of the surveys show an increased support for CER over time (Figure 1). The percentage of physicians stating they strongly support and somewhat support CER increased by 20 points, from 52% to 72%, between 2009 and 2011. As CER continues to evolve and expand from a concept to something more concrete that can be used and implemented, one can expect this trend to continue over time. It is interesting to note that the change observed between the two rounds of surveys came mostly from physicians who back in 2009 reported neither support nor oppose. This particular group went from 29% in 2009 down to 12% in 2011, suggesting that more information on what CER is and does might have helped convince some physicians in regard to its usefulness in their practice.
In all of the situations presented to them, more than 50% of the respondents stated they would be very likely or extremely likely to implement CER (Figure 2). However, more support was observed for shared decision-making with patients and preventive care recommendations where 68% of the physicians said they would be very likely or extremely likely to implement. Between 56% and 58% of the respondents supported the implementation of CER for diagnostic imaging, prescribing decisions, and recommendations for surgical procedures. Still, a significant proportion (32-35%) of physicians stated they were somewhat likely to implement in these situations (compared to 28% to 29% for shared decision-making with patients and preventive care recommendations), indicating a need that more work remains to be done to convince physicians of the applicability of CER in these situations.
Conclusions
To date, little comparative effectiveness data have been available in the diagnostic imaging arena. This void has opened the door to less transparent types of technology evaluations and opportunities for radiology benefit managers to limit access to certain diagnostic imaging tests. The data from Harris Interactive demonstrate a heightened interest in CER as a technology assessment tool for the referring physician. And in order to best serve the needs of referring physicians and payors, and increase adoption of new technology, radiology should be prepared to demonstrate the value of imaging with comparative effectiveness data. It is anticipated that as properly conducted comparative effectiveness studies in radiology become available, the referring physicians will be interested in the study findings. This presents an educational opportunity for the imaging department and radiologists to work closely with the referring physician base and payors to ensure the right test is done at the right time and to improve patient care.
Patrick Bonnet, PharmD, MS, serves as a Director of Healthcare Economics at GE Healthcare. He may be contacted at . Christine Hughes is the Advocacy Research Leader on the Healthcare Economics team at GE Healthcare and may be reached at . Debra Richman is Senior Vice President, Healthcare Business Development & Strategy for Harris Interactive, and may be reached at .
References
- Institute of Medicine. Report brief: Initial national priorities for comparative effectiveness research. www.iom.edu/cerpriorities. Accessed January 27, 2012.
- The Patient-Centered Outcomes Research Institute (PCORI). www.pcori.org/. Accessed January 27, 2012.
- Pandharipande PV, Gazelle GS. Comparative effectiveness research: what it means for radiology. Radiology. 2009;253:600?605.
- Rawson JV. Comparative effectiveness research in radiology: patients, physicians and policy makers. Acad Radiol. 2011;18:1067?1071.

