An ahead-of-print
article in the April issue of the American Journal of Roentgenology
reviewing various techniques and clinical management paradigms to treat severe
frostbite injuries—relevant for interventional radiologists, especially—showed
promising results using both intraarterial (IA) and IV tPA (tissue plasminogen
activator) to reduce amputation.
“Severe frostbite injuries can lead to devastating outcomes with loss of limbs
and digits, yet clinical management continues to consist primarily of tissue
rewarming, prolonged watchful waiting, and often delayed amputation,” write
Boston Medical Center radiologists John Lee, MD, and Mikhail Higgins, MD, MPH.
A search of the literature by Lee and Higgins yielded 157 citations. After
manually screening for inclusion criteria of case reports, case series, cohort
studies, and randomized prospective studies that reported the use of tPA to
treat severe frostbite injuries, 16 qualified for review.
Lee and Higgins’ analyzed series included 209 patients with 1109 digits at risk
of amputation treated with IA or IV tPA—116 and 77 patients, respectively. A
total 926 at-risk digits were treated with IA tPA and resulted in amputation of
222 digits, for a salvage rate of 76%. Twenty-four of 63 patients underwent
amputation after IV tPA, resulting in a 62% salvage rate.
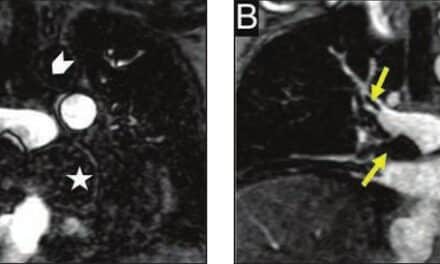
Both digital subtraction angiography (DSA) and triple-phase bone scan were
utilized for initial imaging evaluation of patients with severe frostbite
injuries. Additional concurrent treatment included therapeutic heparin at
500 U/h, warfarin with target international normalized ratio of 2:3,
nonsteroidal anti-inflammatory drugs, pain management, and light dressings with
topical antimicrobial agents.
“For many years,” Lee and Higgins conclude, “the axiom ‘frostbite in January,
amputate in July’ was an accurate description of the common outcome in
frostbite injuries. Through a meta-analysis of thrombolytic therapy in the
management of severe frostbite, this article provides a useful guideline for interventional
radiologists, including a suggested protocol, inclusion and exclusion criteria,
and potential complications.”
What Interventional Radiologists Need to Know About Frostbite and Amputation