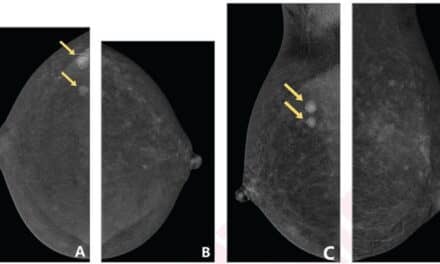
PHOTO CAPTION: Fluorescence images of breast tumor and surrounding normal tissue. Mice bearing breast tumors expressing iRFP were injected with ICG-p28, intravenously. Twenty-four hours later, fluorescence images of the tumor and surrounding normal tissues were recorded. The dotted circles indicate the outer edge of the tissue. Green: ICG-p28, red: iRFP, yellow-orange: colocalization. (photo credit: Yamada laboratory at the University of Illinois at Chicago)
Nearly 13 percent of women born in the U.S. today will develop breast cancer at some point during their lives. Treatment for early-stage disease often includes breast-conserving surgery, where the breast tumor and some surrounding healthy tissue (the tumor margin) are removed. However, around 20 percent of these surgeries require a second operation, generally because cancer cells are found within the tumor margins.
Now, NIBIB-funded researchers are developing an imaging method that would allow surgeons to better identify cancerous cells in the tumor margins during surgery. This technique could lead to a reduction in follow-up breast cancer surgeries and reduce rates of breast cancer recurrence. Results were recently published in eBioMedicine, a publication of The Lancet.
“Today, surgeons primarily rely on their sense of sight and touch to distinguish between healthy and cancerous tissues during surgery, which may lead to incomplete removal of the tumor,” said Tatjana Atanasijevic, PhD, manager of the NIBIB program in Molecular Probes and Imaging Agents. “This imaging technique provides real-time visual feedback during surgery, allowing surgeons to better gauge the breast tumor margins, and ultimately optimizing surgical excision.”
The technique relies on a method known as near-infrared imaging, which utilizes probes that fluoresce under near-infrared light. These fluorescent probes can allow clinicians to visualize features beyond the tissue surface, such as blood vessels or tumors, which can help to guide surgical procedures. However, there aren’t many near-infrared agents that are approved for clinical use by the U.S. Food and Drug Administration (FDA), and those that are approved are non-specific, meaning that they don’t home in on a specific target in the body. Further, the only near-infrared probe approved for surgery, indocyanine green (ICG), doesn’t stay in the bloodstream for very long and therefore its utility for image-guided tumor resection is somewhat limited.
To overcome the limitations of traditional near-infrared imaging probes, researchers from the University of Illinois at Chicago have designed a new probe specifically designed to detect cancerous cells within breast tumor margins in real time during surgery. This probe combines the FDA-approved dye ICG with a non-toxic, tumor-targeting, cell-penetrating peptide known as p28.
“Our research group has previously reported that p28 preferentially enters into various human breast cancer cells and actually induces anti-proliferative effects,” explained Tohru Yamada, PhD, an associate professor in the Department of Surgery at the University of Illinois College of Medicine and senior author of the study. What’s more, p28 has been evaluated in early clinical trials and was well tolerated by patients. “Our new probe, termed ICG-p28, can selectively illuminate breast cancer cells under near-infrared light and thereby facilitates the image-guided removal of cancerous tissue at the time of surgery.”
The researchers first needed to determine how well their imaging probe could accurately delineate breast cancer from healthy tissue. To do this, they created a breast cancer cell line that expresses a protein called iRFP, which fluoresces under near-infrared light. This way, when the researchers establish their breast cancer models by injecting mice with this particular cell line, they can precisely visualize the exact shape and size of the breast tumors.
After establishing the breast cancer models, the researchers then injected the mice with their imaging probe, waited 24 hours, excised the tumors, and compared the fluorescent signals between iRFP and ICG-p28. They found that the two signals had excellent overlap, indicating that their imaging probe specifically targets breast cancer tumors for an extended period of time.
Next, Yamada and colleagues used their probe to guide tumor resection in two models of breast cancer and watched the animals for cancer recurrence. Once the mice developed tumors, the researchers injected them with either ICG-p28, ICG alone, or a control buffer solution without any near-infrared dye, and waited 24 hours.
Then the tumors were removed, aided by image-guided visualization using near-infrared light, or using traditional palpation and direct visualization (for mice injected with the control buffer solution). Four weeks after the surgery, more than 30% of mice injected with the control buffer solution experienced tumor recurrence, and 25% of mice injected with ICG alone experienced recurrence. However, just over 6% of mice injected with ICG-p28 experienced recurrence, demonstrating that the ICG-p28 probe improved surgical outcomes.
“This preclinical study demonstrated that intraoperative imaging with ICG-p28 can accurately identify tumor margins and ultimately improves the tumor recurrence rate in multiple breast cancer models,” said Yamada. “Additionally, because p28 preferentially penetrates various types of human cancer cells, we anticipate that our imaging approach can be applied to additional cancer types.”
Yamada noted that this research is still in the early stage, and that the evaluation of this imaging probe in a clinical trial will be an important next step to determine how well it works in human patients.
[Source(s): National Institute of Biomedical Imaging and Bioengineering, Newswise]