A non-invasive, patient-friendly imaging technique can help physicians make treatment decisions for breast cancer patients when diagnostic dilemmas arise. The 18F-FES PET scan—approved by the U.S. FDA in 2020—was shown to solve 87% of dilemmas, providing physicians with information for personalized treatment decision-making. This research was published in the September issue of The Journal of Nuclear Medicine.
A key characteristic of breast cancer is the estrogen receptor (ER), which is expressed by 79% of breast tumors. Breast tumors that are ER-positive are likely to respond to hormonal therapy. To assess the presence of the ER, a biopsy of a tumor or metastases is commonly performed. However, clinical dilemmas may arise when a biopsy cannot be performed safely or when discrepancies in ER expression is suspected between tumor lesions.
“18F-FES PET has the potential to visualize the ER expression of all tumors across the body, and could provide helpful information regarding clinical dilemmas in breast cancer patients,” says Carolina P. Schröder, MD, PhD, a medical oncologist at the University Medical Center Groningen in The Netherlands. “In our study, we evaluated whether ER clinical dilemmas could be solved by 18F-FES PET findings.”
The retrospective study reviewed 100 18F-FES PET scans that were performed on 83 patients with three types of clinical dilemmas. These dilemmas included the inability to determine the extent of disease with the standard workup, unclear ER status of the tumor, or the inability to determine which primary tumor caused the metastases.
18F-FES PET solved the clinical dilemma in 87% of scans. In 93% of the solved cases, a treatment decision was based directly on the 18F-FES PET result. The frequency of solved dilemmas was not associated with the type of dilemma. However, the frequency of solved dilemmas was related to ER status, as dilemmas in ER-positive scans were more likely to be solved than in ER-negative scans.
“This is the largest study to show the value of 18F-FES PET in a ‘real daily clinical practice,’” says Schröder. “These findings support the use of 18F-FES PET for optimal patient outcomes and may support broad implementation of 18F-FES PET in clinical practice.”
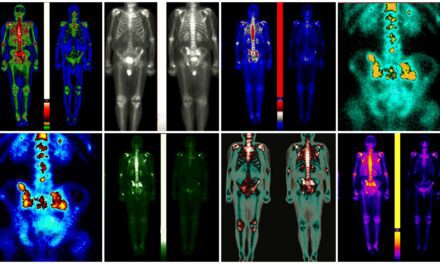
Featured image: Determination of ER status of disease. In 59-y-old woman diagnosed with ER-positive lobular BC 2 y previously and treated with tamoxifen, ER-positive bone metastases were identified 1 y after initial diagnosis. She was treated with first-line endocrine therapy in palliative setting. Thereafter, disease became progressive and palbociclib was added. However, after 2 wk of treatment, she presented with pancytopenia. 18F-FES PET was performed to determine whether bone metastases were still expressing ER and whether there was a rationale for another line of endocrine therapy. Increased 18F-FES uptake could be seen in lymph nodes above and below diaphragm and in multiple bone lesions (e.g., spine, costae, scapulae, sternum, and pelvis) (A, maximum-intensity-projection image; B, PET/CT sagittal view; C, PET/CT transversal view of left axillary region; D, PET/CT transversal view of pelvic region with positive inguinal lymph node). In addition, bone marrow involvement was visible. Diagnosis was settled on ER-positive metastatic disease, clinical dilemma was solved, and another line of endocrine therapy could be considered. However, because of bone marrow involvement, chemotherapy was indicated to achieve therapeutic effect more rapidly.