Breast tissue features apparent on MRI are linked with future second breast cancer risk in women with a personal history of breast cancer, according to a study published in Radiology, a journal of the Radiological Society of North America (RSNA). Breast cancer is the most diagnosed cancer and the leading cause of cancer-related death in women worldwide. While advances in treatment and early detection mean that more women are surviving breast cancer, these women face an increased risk of second breast cancers.
Breast cancer survivors with dense breasts face an even greater risk of a second cancer. Breast tissue is mostly fatty, with areas of fibrous connective tissue and glandular tissue known collectively as fibroglandular tissue. Women with dense breasts have a greater proportion of fibroglandular tissue and less fatty tissue. This can obscure lesions on mammography and is an independent risk factor for breast cancer.
Breast MRI has become the preferred method for imaging women with personal history of breast cancer. Previous studies have shown that breast MRI has a higher cancer detection rate than mammography.
“Postoperative surveillance breast MRI is increasingly being performed according to the American College of Radiology’s annual recommendation for women with dense breasts or those diagnosed with breast cancer before age 50,” says study lead author Su Hyun Lee, MD, PhD, from the department of radiology at Seoul National University Hospital in Korea.
Lee and colleagues studied the link between second cancer risk and background parenchymal enhancement (BPE) at surveillance breast MRI. BPE refers to the brightening, or enhancement, of background tissue on MRI after administration of a contrast agent. The degree of BPE can vary between and within women. It is thought to be related to changes in the blood supply and permeability of breast tissue, which is affected by hormonal status. Breast cancer treatment in the form of radiation therapy, chemotherapy or endocrine therapy can also alter the BPE in the treated breast.
BPE on contrast-enhanced breast MRI is a known risk factor for breast cancer. Less is known about the links between BPE at surveillance breast MRI and the risk of second breast cancer.
Of the 2,668 women in the study, 109 developed a second breast cancer at a median follow-up of 5.8 years. Mild, moderate, or marked BPE at surveillance breast MRI was independently associated with an increased risk of future second breast cancer compared to minimal BPE.
“The results suggest that BPE at postoperative surveillance breast MRI may indicate the response to breast cancer treatment and may be a predictor of the modified risk of second breast cancer after treatment in women with a personal history of breast cancer,” Lee says. The study findings point to a role for BPE measurements in refining screening pathways for women with prior breast cancer, Lee says.
“Our study results may help to stratify the risk of second breast cancer in women with a personal history of breast cancer and to establish personalized imaging surveillance strategies in terms of imaging modality and monitoring interval selection,” she says. “For example, women with minimal BPE at surveillance breast MRI may no longer need to undergo contrast-enhanced breast MRI every year if other risk factors are absent.”
Those other risk factors include younger age at diagnosis, the presence of genetic mutations linked to breast cancer and hormone receptor expression in the initial breast cancer.
Areas for future study include the link between BPE changes at screening or preoperative breast MRI and at postoperative surveillance breast MRI and the development of second breast cancer.
In the future, Lee expects that risk models will use mammography, ultrasound, and MRI together. This approach, she says, will lead to more tailored surveillance strategies for women with a history of breast cancer.
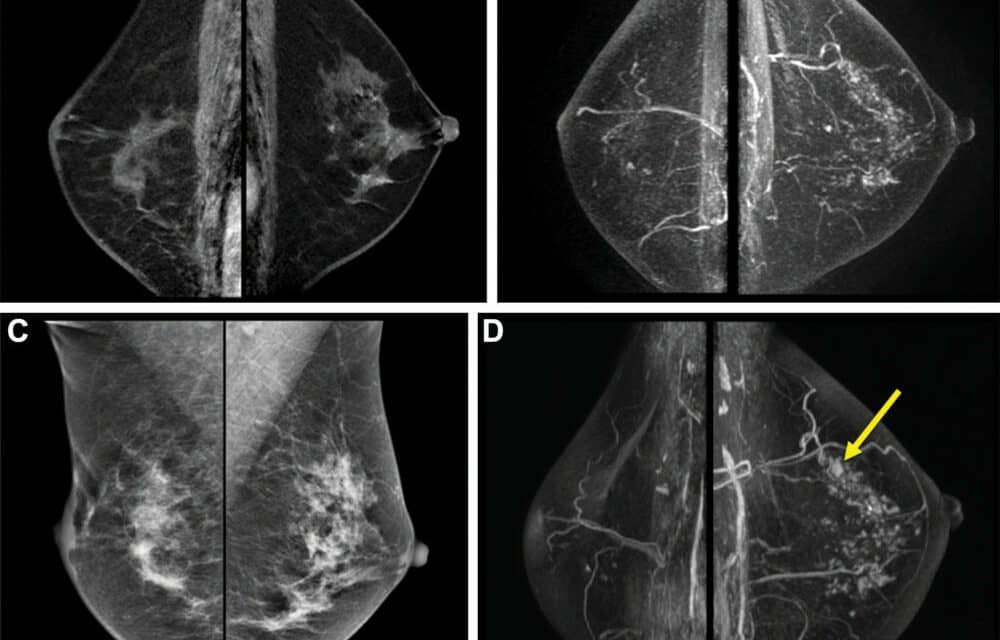
Featured image: Figure 3. Postoperative surveillance images in a 54-year-old woman who had undergone right breast–conserving surgery and postoperative radiation therapy 2 years prior for stage III hormone receptor–positive invasive ductal carcinoma. She had completed adjuvant chemotherapy and was on endocrine therapy. She had no family history of breast cancer and had not been tested for the BRCA1/2 genes. (A)Bilateral sagittal contrast-enhanced T1-weighted and (B) maximum intensity projection images from baseline surveillance breast MRI show asymmetric moderate background parenchymal enhancement in the left breast. (C) Surveillance mammograms acquired within 6 months of surveillance breast MRI show heterogeneously dense breasts. (D) Subsequent surveillance breast MRI scans acquired 2 years after baseline surveillance breast MRI show a small irregular enhancing mass in the left upper breast (arrow). Biopsy and surgical pathologic examination revealed a 0.8-cm ductal carcinoma in situ.



