The Centers for Medicare and Medicaid Services (CMS) and commercial payors are determined to put a lid on growing diagnostic imaging utilization and reimbursement levels. Diagnostic imaging is one of the fastest-growing cost areas in American health care, and the growth in advanced medical imaging as a major contributor to today’s exploding Medicare spending is well documented. Outpatient diagnostic imaging spending exceeds $100 billion and is growing at a rate in excess of 20%. Commercial payors nationwide report double-digit growth in advanced imaging and question the appropriateness of advanced imaging orders.
CMS and commercial payors are well under way in taking steps to curb imaging utilization and reduce reimbursement by implementing:
- cost-efficient radiology management programs;
- pay-for-performance (P4P) contracts;
- multiple-procedure reduction on contiguous scans;
- caps to the imaging technical payment at the lesser of Physician Fee Schedule or hospital outpatient rate; and
- proposed revision on the CMS work and practice RVUs, reducing radiology reimbursement 4.3% to 12.1%.
Payors also are trying to limit the number of service sites by forcing accreditation of imaging centers using specific criteria prior to contracting sites to provide services to enrollees. Accreditation standards include criteria ranging from requiring a 40-hour minimum of weekly operation to having available a minimum number of imaging modalities.
It is anticipated that imaging centers around the country will experience cuts by as much as 50% for some MRI procedures with per-scan revenue losses exceeding $400. Although Congress estimates the measure would save $2.8 billion over 5 years, the American College of Radiology (ACR), Reston, Va, puts this figure at closer to $6 billion.
While CMS focuses on the reimbursement rates of imaging, commercial payors will continue to focus on controlling imaging utilization by adopting management programs and P4P contracts with imaging providers. The utilization management programs have demonstrated some effectiveness in combating double-digit volume inflation and have become very popular as a solution to curbing runaway costs and inappropriate ordering of imaging examinations.
Radiology management companies (RMCs)—such as National Imaging Associates/Magellan (NIA), Avon, Conn; MedSolutions, Franklin, Tenn; CareCore National, Wappingers Falls, NY; and American Imaging Management Inc (AIM), Deerfield, Ill—claim they can reduce inappropriate ordering of high-tech imaging procedures by educating referring physicians. These companies are contracted by payors to manage their radiology services with the expectation that utilization of high-tech imaging procedures will be reduced. Indeed, many of these payors have already reported significant returns in contracting with radiology management companies.
The Independence Blue Cross Affiliate Company Pilot Program had a growth rate of 17.4% for CT; after contracting with AIM, the growth rate is now .9% and 0.2% for MRI. CareCore has advertised the reduction of utilization rates by 3% to 5%.
P4P contracts also have been adopted by some commercial payors to help curb utilization of high-tech imaging procedures. Payors are contracting with physicians and hospitals to hold 5% to 15% or more of allowable or contracted fees. This plan is designed to encourage hospitals and physicians to control utilization while maintaining high-quality patient care. Several patient-care specifications are negotiated and ranked among all specialties, including primary care and ancillary departments. The most popular initiative is measuring utilization of high-tech imaging services. However, these programs have proven to be difficult to manage for both the payor and the providers and hospitals. It is difficult to measure radiology utilization because of data collection challenges, clinical protocol changes, technical advancements, coding and billing changes, or “utilization creep.” It has been difficult to develop meaningful and easy provider measurements to benchmark performance. The participation costs for hospitals may be greater than the P4P payout.
Revenue Protection Mandate
It is becoming increasingly important for imaging centers and hospitals across the country to protect their revenue and to position their practices and operations for the inevitable, particularly in protecting revenue from the RMCs. These companies may help curb utilization, but they are imposing significant operational costs on hospital radiology departments, radiology practices, and imaging centers across the country. In July 2006, the Radiology Business Management Association (RBMA), Irvine, Calif, conducted a mini-survey to measure the impact the various utilization reduction programs as well as the DRA cuts have or will have on its membership. The survey reported that 92.8% of the respondents have payors who require a precertification for outpatient nonemergent imaging. The top modalities requiring a precertification included MRI, CT, PET, and nuclear cardiology. A total of 83.1% reported having to change internal or external procedures to ensure the procedure is properly precertified prior to performing the examination. Although the radiology management companies advertise that no additional cost is imposed on the radiology provider, 65.5% reported they had to hire additional personnel or incurred additional operational costs to assist in the precertification process; 138 respondents participated in this survey.
 |
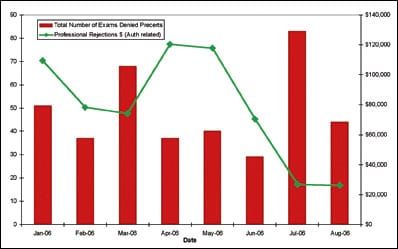
| Figure. Number of examinations with unattainable precertification vs professional authorization-related rejections. |
Managing High-Tech Imaging Internally
The department of radiology at Massachusetts General Hospital (MGH), Boston, and Radiology Associates, Boston (physician organization), both recognized the need to take matters into their own hands to manage the precertification process. The goal was to avoid tremendous losses due to administrative hassles that the precertification and P4P programs could impose on them.
MGH and Radiology Associates imaging centers bill more than 3,000 procedures per day, and it would be impossible to manage each procedure for precertification and appropriate ordering manually. With the guidance of Partners HealthCare Information System (IS) teams, radiology IS, and a radiologist, a Web-based online Radiology Decision Support System (DSS) was developed. The DSS has become one of the major components in the management of the P4P programs. The DSS educates the physician on the appropriateness of ordering high-tech procedures using ACR appropriateness criteria and many years of outcome results based on ICD-9 codes and signs and symptoms. The DSS has become a very important tool in the precertification process as well.
Many payors have recognized this as a good tool in educating physicians on the appropriateness of ordering radiology procedures and curbing utilization. The MGH referring physician orders the radiology examination through a radiology order entry (ROE) system that is available via the intranet. The decision support module provides the referring physician with a green, yellow, or red score indicating the appropriateness of the procedure they are ordering for their patient’s diagnosis, sign, or symptom. The yellow and red indicators educate the referring physician on the inappropriateness of the examination they are ordering and offer alternative procedures for their patient’s condition. On a weekly or monthly basis, the referring physician’s department or section chief is given a report card depicting their physician’s or clinic’s ordering patterns and benchmarking them against other physicians who order radiology procedures within the MGH network. The radiology department also meets with the referring physicians using ACR or MGH radiology clinical protocols, which are based on well-documented outcomes, to help them achieve better ordering appropriateness.
When a score is given and the patient’s procedure is ordered electronically, the procedure is “screen scraped” (copy/pasted) into the RIS. The procedure is flagged if a precertification is required based on the patient’s insurance information obtained from the hospital’s registration system via an electronic gateway. If the order does require a precertification and the procedure was ordered in ROE, special arrangements were made with three major payors to use an electronic home-grown gateway to the payor to get an authorization, thus avoiding the need for the referring physicians to contact the RMCs directly. This process takes away the burden from the referring physician and allows radiology to obtain the precertification with the least amount of administrative hassle. This process was accomplished only by selling the payor on the decision support system and the ability to monitor the appropriateness of ordering radiology procedures internally and share the results with the payor via the P4P contracts.
Managing the Precerts
MGH is a very large organization, and many referring physicians outside of its network do not use ROE. In this case, the department of radiology worked collaboratively with the professional and hospital billing offices to develop a home-grown tool to manage the precertifications and try to minimize the administrative burden the processes impose on them. Using a SQL server and Microsoft Access, a database was designed to store and monitor precertifications by payor, encounter, and CPT code.
The precertification database is updated twice a day—once in the morning and once in the afternoon. At these times, a report is run and information from the RIS is downloaded into the precert database. The download collects examination information based on outpatient examinations scheduled for the upcoming 7 days as well as the previous 4 days. Information is collected only for predesignated examination types and payors. The information is then added to the database, and the manual effort begins. Currently, MGH Radiology Scheduling Representatives (RSRs) take on the responsibility of getting precertifications for examinations that were ordered without one. Depending on the payor, this is sometimes done by going to Web sites or calling payors on the phone; however, more often than not, it requires a call to the front desk staff of the ordering physician. This process is time-consuming and labor-intensive, and it requires staff to be knowledgeable about a vast number of different payor criteria and processes by which the precertifications are obtained.
Currently, MGH works with three radiology management companies and more than seven payors that use these companies. Each payor and radiology management company uses different rules in managing their programs (see Table).
 |
| It is becoming increasingly important for imaging centers and hospitals around the country to protect their revenue and to position their practices and operations for the inevitable, particularly in protecting revenue from the radiology management companies. — Christie James, MS |
It is a formidable challenge to manage the administrative failure points in the precertification process unless you have the tools to help you manage them. The failure points that have been identified over the last year include:
Precertification validations. Precertification requests are valid 30 to 60 days from the date of service depending on the payor. This becomes problematic if the examination is rescheduled prior to the start date of the authorization validation period. A report is run 7 days prior to the date of service and is matched up with the database to identify any rescheduled examinations. The MGH staff follows up with the PMCs to ensure the precertification is revalidated.
CPT and precertification authorization mismatch. The patient’s procedure is changed at the time of scanning. This is very common in hospital settings because the patient’s imaging protocol is changed depending on the clinical history available at the time of scanning. A daily report is run from the RIS to identify any procedure changes or add-on procedures that differ from the original order. These order changes are discussed with the referring physician and documented in the RIS. The precertification management staff notifies the RMC for revalidation post examination.
Secondary insurance companies require precertifications, and the referring physician is not aware of this at the time of obtaining the precertification. MGH staff continuously educates the referring physician office on which primary and secondary payors require precertifications. A payor precertification grid is on the MGH Radiology Web site, and radiology’s marketing team also trains and distributes this to the referring physician offices.
A different precert number is required for each CPT code billed. Some payors require only one, and it covers up to 12 CPT codes, while others need a separate precertification for each CPT. The database enables the staff to easily identify these when securing authorizations for the next day or future appointments.
Add-on or walk-in procedures are sometimes missed in the precertification management process. The daily reports for the precertification database identify these, and a call is made to the referring physician or RMC for precertification.
Many payors will require a precert for the technical component only, and some require a separate precertification for the technical component and one for the professional component. A precertification always is required for the global procedure at the physician-owned imaging centers, which includes both the professional and technical components of the procedure.
Select payors require a precertification for a precise CPT code without giving any consideration for family or grouping of codes, such as CT head without contrast, CT head with contrast, and CT without and with contrast. Referring physicians or their assistants sometimes do not know whether the patient will receive contrast for the procedure they are ordering. It is up to the radiology department to ensure the RMC has the correct CPT code authorized. The radiology precertification team has 48 hours after the procedure to notify the RMC of the correct CPT charged to avoid denial.
In a hospital setting, a claim can be passed onto the payor as either inpatient or as an emergent case and denied for no authorization. A robust denial management process should identify these and appeal to the payor as needed.
Patient’s insurance changes from the time the procedure is ordered and the actual date of service. Staff needs to reconfirm the status of the insurance and obtain the new precertification if required.
Precertifications may not be valid for your place of service or may contain bogus precertification numbers. All precertifications should be validated using the RMC or payor Web sites.
The precertification management staff runs several management reports from the database and the radiology schedule to identify the above failure points and correct them as they are identified.
Tracking the Effort
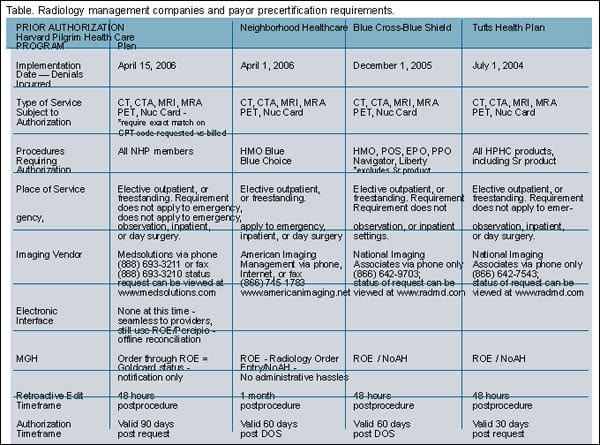 |
| Table. Radiology management companies and payor precertification requirements. (click image for larger view.) |
Over the past year, this process has been modified and refined a number of times by a multifunctional group representing all areas of the process, including operations, billing (both technical and professional), scheduling, marketing, and information technologies and programs. Now that some level of consistency has been achieved, the focus has shifted somewhat from the day-to-day operations of the system to a monitoring phase to spot trends and determine if further adjustments need to be made. The precertification management team developed key performance indicators to assist in following trends and other failure points in the precertification management process.
The group determined that three areas needed to be tracked: number of encounters worked in the database, how many procedures missed the database altogether, and the actual number of procedures that were rejected for no authorization or other types of rejections. These all needed to be reported to begin to adequately represent the management of the precertification process and to identify any major issues that might arise. It also was determined to measure performance in monthly intervals to compare and trend data.
The precertification database was a natural area that needed to be covered because MGH needed to ensure that the examinations, which had been identified as needing precertifications, were actually getting them. Its usefulness extended further as the system was used by the hospital and professional billing offices to appeal denied claims. All encounters that are entered into the database had either a precertification authorization or a reason why one was not obtained. There are 10 different options, including “not medically necessary” and “exhausted efforts.” The top five examinations and ordering physicians without precertifications also were tabulated so that the radiology marketing team could reach out to the physicians who ordered examinations without precertifications so that their staff members could be educated on the process to avoid further denials.
Denial Management Is Essential
Denial management is a critical part of this process and requires feedback from both the professional and hospital billing offices to ensure that failure points are consistently monitored and processes changed to avoid unnecessary denials. Monthly or weekly reports should be monitored by payor and rejection code to identify the rejections for:
- no-authorization;
- date of service does not match date of authorization;
- authorization not valid for CPT code; or
- medically not necessary or the procedure is not valid for the ICD-9 code billed.
A root cause analysis should be performed on each of the rejections to determine where the failure points are in the precertification process. Some of the problems identified were as simple as the ordering physician’s office (usually the secretary) ordered a CT of the chest and CT angiography or cardiac CT was performed. The CPT code is not changed prior to the date of service; thus, the authorization is not valid for the examination performed. Marketing educates the ordering physician’s office and the online ROE is modified to minimize ordering mistakes.
Radiology management companies also can provide an authorization, and the payor can still reject as not medically necessary according to their local medical policies. This type of rejection puts a tremendous administrative burden on the referring physician’s office as well as the radiology precertification and denial management teams. The payors have the ability to deny the claims based on ICD-9 code, and the patient is not held liable (for MGH’s negotiated contracts). It is important for the radiology practice to be aware of its local payor policies, educate scheduling staff, and keep online ordering systems updated on payor payment policies to help educate the referring physician’s office.
Conclusion
The administrative burden resulting from precertification programs and financially motivated P4P contracts has undoubtedly added additional operational costs to hospitals, radiology practices, and billing offices nationwide and lined the pockets of the RMCs. Hospitals and radiology imaging centers across the country are beginning to report losses for no-authorization denials and are unable to develop internal work processes to ensure an authorization is secured at the time the procedure is performed. Many RMCs cannot understand why there are so many problems with securing a precertification at the time of ordering the examination. It is not that the hospital or imaging center cannot obtain a precertification at the time of scheduling the examination. The problem lies in the administrative changes that occur from time of order to time of billing and payment or denial. Providers also are saddled with the divergent policies of both payor and RMC precertification rules.
Christie James, MS, is radiology billing manager, and Kenneth R. Lamy, MBA, is reimbursement analyst, Massachusetts General Physicians Organization, Charlestown, Mass, affiliate of Massachusetts General Hospital and Partners Health Care Network, and Bert Nagtegaal, MBA is project specialist, quality management and education, Massachusetts General Hospital Department of Radiology, Boston.



