The concept of time of flight for positive electron tomography (PET) is not a new idea. It has been around for the last 40 years, including a less-than-successful spate of research a quarter century ago.
With the development of more powerful computers, state-of-the-art materials, and new algorithms, Philips Medical Systems, Andover, Mass, was able to successfully implement time of flight in its Gemini TF. The machine was released to the market in November 2006.
As with any new technology, a launch does not mean that it has found a niche in the medical community. After 1 year, it is time to discover whether time of flight has found a home in the radiology department.
Physics Lesson
Philips’ technology, which the company calls TruFlight, differs fundamentally from a conventional PET machine. In conventional PET imaging, a lesion can be detected, but not its exact location. The result is an image that is “noisier,” said Joel Karp, PhD, professor of radiology at the University of Pennsylvania.
Though conventional PET is better than planer radiology in that it is not limited by overlying images, it is not as accurate as that available in time of flight. Karp explains this is because though conventional PET can image along a line showing the equivalent of a back-and-front projection of the view, it cannot pinpoint a lesion. This is solved with time of flight. “You can localize the timing,” he said. “It reduces the distance along which you’re doing the projection, and, as a result, reduces the noise.” According to Karp, the timing resolution is about 600 picoseconds with an uncertainty of about 9 cm.
The results are not only in better localization and diagnosis, but in images that are “absolutely spectacular,” said Robert Henkin, MD, professor emeritus of radiology at Loyola Stritch School of Medicine, Chicago. “There is better precision because of the better quantification.”
Karp agrees that image quality is the most relevant aspect of the time of flight technology. He notes that the Gemini allows for reconstruction with higher contrast but without an increased ratio of “noise” or scatter. From a qualitative perspective, he said that reconstructing the multiple views gathered from the PET depends on how much information is captured. “It is better if it’s localized information instead of information from all over,” he said.
The improved imaging is better and safer for the patients. There has been no need to increase either the radiation or contrast patients need to experience.
The physics forming the basis for the more accurate PET time of flight images are successful in the abstract. But it took Philips to translate these into a successful package—the Gemini TF.
 |
| The primary diagnostic uses for Philips’ Gemini are oncology, cardiac, and neurology. |
Twinned Machine
Not surprisingly, the Gemini TF looks like a large computed tomography (CT) device with a bore of 73 cm. The footprint is similar to Philips’ competitors’ machines measuring 16 feet x 24 feet. “That’s pretty much the industry standard,” said Peter Cempellin, general manager, Philips Nuclear Medicine/PET.
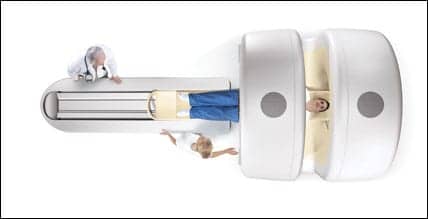
Having time of flight capability is not the only unique aspect about the Gemini. According to company promotional materials, because it has the combination of PET and CT, it has improved “diagnostic correlation.” The CT is available in either 16- or 64-slice versions. The machine’s design is unusual in the fact that patients undergo the PET and CT at the same time. The patient is placed on a long gantry, their hands over their head holding a grip bar. They are then fed into the machine and imaged first with the CT and then with the PET. There is an open view between the two gantries, which makes it much more comfortable for patients. “It alleviates a lot of the problems associated with claustrophobia,” Cempellin said.
The Gemini has a number of unique features that, according to Karp, make it possible for the device to deliver time of flight effectively. These include the LYSO scintillator; the device’s geometry, which measures 4x4x22 mm (the 4×4 mm gives it better spatial resolution; the 22 mm gives the optimal balance between resolution, sensitivity, and cost, according to the company); the PIXELAR detector design, which was selected for better 3D performance; and better energy resolution.
In addition to the detectors, the system also comes with a computer system based on the company’s Brilliance workstation. It is fully DICOM and PACS compatible.
The primary diagnostic uses for the Gemini are oncology (93%), cardiac (4%), and neurology (3%).
Cempellin describes the cost of the Gemini TF as “competitive.” Henkin estimates that it costs about 20% more than a conventional PET (“Its only downside,” he said).
Cempellin acknowledges that, because of the budgetary realities of modern health care settings, radiology departments might not be able to afford implementing time of flight in a single purchase. The company offers a time of flight-ready version of the Gemini. “It’s an attractive option,” Cempellin said. This option is designed primarily for two scenarios. The first, for the department that has budgeted for a new PET machine, but not the extra premium price for time of flight—which then can be budgeted during the next purchasing cycle. The second, for the department that does not have the volume, as of yet, to support it, but may in the future.
The operating interface is based on a Windows platform. “It’s intuitive, easy to use, and icon driven,” Cempellin said.
The company has about 56 Gemini TF machines in place with orders for about 30 more. There are three primary customer types that buy the Gemini TF:
- Large luminary research medical centers;
- Medium and large-size hospitals with high patient volumes; and
- Small entrepreneurial practices looking for a competitive edge.
Gemini in the Field
Saint Louis University, St Louis, which has a 340-bed hospital, was among the first users of the Gemini TF.
Saint Louis University has been using Philips’ Gemini since 2004 and the TF variant since late 2006. The university purchased the 64-slice CT option along with the TruFlight technology.
The university has been experiencing rapid growth in its need for PET with demand increasing by about 20% per year from 1,000 studies in 2004 to a projected 1,800 for 2007. The university needed a fast, accurate machine. According to Medhat M. Osman, MD, ScM, PhD, an associate professor and director of nuclear medicine and PET/CT, the Gemini TF has delivered. “It’s working very nicely for us,” Osman said. “We can scan from the skull to the upper thigh in about 9 minutes, which is three times faster than a conventional PET scan.”
In addition to the faster speed, Osman said that the sensitivity and precision of the time of flight technology allows him to find lesions that are significantly smaller. “We used to look for lesions that were 6 mm to 7 mm. Now, we can see ones that are smaller,” he said, adding that this gives him and his colleagues an additional level in comfort for diagnosis.
However, Osman refuses to commit as to whether the Gemini delivers significantly better image quality. “Better image quality is subjective,” he said. “I don’t think there are any bad PET/CTs out there.”
The only downside with the increased sensitivity is that Osman finds he must take as much time or longer to read it than he does to acquire the image.
An unusual aspect of the studies performed at Saint Louis University is that no matter the initial indication, the patient receives an entire body scan.
The radiology department uses the Gemini TF primarily for oncology studies in patients that have a known or highly suspected cancer. The department also uses its Gemini machine to do neurology and cardiology studies. The 64-slice option was chosen primarily to allow for better cardiology studies. Osman said that the CT on the Gemini is currently the best in the hospital.
Though every patient will receive a full-body scan, the department also uses its Gemini just for CT studies alone. For that purpose, the department had all of the technologists who were using the machine cross trained to use it in PET/CT mode and CT mode alone.
The department decided to train the PET technologists and did so with the help of Philips both at Saint Louis University and at Philips’ headquarters in Ohio. According to Philips’ Cempellin, the company-based course combines traditional classroom instruction with hands-on experience. “We take them through all of the parameters,” he said. In this case, after their initial courses the technologists finished their training at the Society of Nuclear Medicine.
Osman describes the effort as wholly collaborative with both the nuclear medicine and CT departments cooperating to make sure the technologists were adequately trained. “It worked out very well,” he said. “The radiology department was very pleased with the results.”
Philips not only offers support by training technologists and radiologists about its equipment, but, after purchase, supports its product as well.
Company Support
 |
| Experts say that improved imaging with time of flight PET/CT is better and safer for patients. There is no need to increase radiation or contrast. |
Osman said that the Gemini TF has been very reliable. The department schedules regular preventive maintenance with Philips. When the scanner has gone down, technicians were dispatched the same day to repair it.
Cempellin said that the company has 4,000 technicians throughout the world who can respond to a client within 4 hours. The Gemini TF comes with a warranty for the first year. After the warranty expires, the company offers a maintenance contract.
Most service calls—80% according to Cempellin—can be handled by the Philips’ phone support staff. “Most of these issues are handled satisfactorily by the response center and is usually an issue of the application and training,” Cempellin said.
The company also maintains a remote service network, which allows technicians to dial in to the site’s computer and study the error logs. In this way, the technicians can diagnose the problem and determine if it can be troubleshot over the phone or if a service person needs to be dispatched.
Service, reliability, and high throughput make the Gemini TF an attractive piece of equipment. But it has another card up its proverbial sleeve that makes it even more useful in this day and age—its ability to provide superior imaging of obese patients.
Heavier Patients
The University of Pennsylvania’s Karp explains that the better image quality in obese patients was understood and predicted as early as the 1980s. The improvement is related to the patient’s overall mass. Taking into account the 9 cm of uncertainty that is typical with time of flight technology, a patient who is 18 cm in diameter, for instance, will have a study that is relatively worse than a patient who is 40 cm in diameter. Because of this, there tends to be less scatter with obese patients with the net result that a lesion can be pinpointed more easily.
Osman, who said about 45% of his patients are obese, agrees that the Gemini TF has advantages over other PET machines in terms of image quality. “Comparing apples to apples, our images [for obese patients] with the Gemini are better,” he said.
Cempellin said that Philips does use the fact of better imaging of obese patients as part of its marketing. However, the company approaches this fact in a broader context, noting that the Gemini has the ability to image all body types. “That’s an enormous benefit to doctors,” Cempellin said.
While the Gemini TF’s first year appears to be a success, there are still improvements that can and will be made in the future.
Next Step
Osman sees the Gemini TF as a significant advance for PET imaging. “It’s a milestone development in PET and just the beginning,” he said. “I expect that it will become faster in the future and I will be able to see smaller lesions. Right now, PET is relatively slower and has a long way to go to catch up.”
One of Osman’s hopes for a future improvement is already on the Philips drawing board. According to Cempellin, CAD will be part of a future iteration of the Gemini. Cempellin foresees other improvements as well, including the introduction of new isotopes that will allow for imaging for more specific diseases.
In the next decade, Karp predicts that there will be further improvement in the materials being used in PET and that will translate into even faster timing on the order of 300 picoseconds.
But most significant is how quickly time of flight has caught on in nuclear medicine. According to Cempellin, one radiologist who uses time of flight has quipped: “If you’re not doing time of flight, you’re not doing PET.”
C.A. Wolski is a contributing writer for Medical Imaging. For more information, contact .



