
 |
| Richard Solomon, MD |
Contrast-induced nephropathy (CIN) continues to be a significant concern for radiologists and cardiologists. Improvements in diagnostic techniques and interventional procedures have led to the performance of more studies with iodinated contrast. In addition, the patients receiving contrast studies are older and have more comorbidities that increase the risk of an adverse renal effect of the contrast media. Despite continuing efforts to reduce the incidence of CIN, a wealth of current data suggests an incidence of 5% or less in low-risk individuals and 15% to 20% in high-risk individuals who are not given any prophylaxis.1
Most data on the incidence of CIN are derived from studies (such as coronary and peripheral angiography) in which contrast is administered intra-arterially. Less information is available regarding the incidence of CIN when contrast is administered intravenously (IV) as part of urography or CT protocols. The table (next page) reviews recent data from prospective studies of patients with baseline renal insufficiency. While the incidence of CIN appears to be less than it is for intra-arterial injections (an average of 13.5% for individuals not given any pharmacological prophylaxis),2 it is still of concern. It is estimated that there are 10 to 20 times more contrast-enhanced CT examinations than coronary angiograms performed each year. Therefore, the absolute number of individuals developing CIN as a result of a CT examination exceeds the figure for coronary angiography.
To minimize the overall risk of CIN, patients at high risk must first be identified. Various risk factors are known to be associated with CIN. Many of these risk factors can be detected using a screening questionnaire that seeks to identify individuals with kidney disease, diabetes, heart failure, and volume depletion. For all of these individuals, more specific information regarding renal function is required in the form of an estimate of glomerular filtration rate (GFR). The most widely used approach relies on the Modification of Diet in Renal Disease (MDRD) formula, which uses serum creatinine, age, gender, and race to estimate GFR. Other formulas, however, may be used, including the Cockcroft-Gault estimate of creatinine clearance. An estimated GFR of less than 60 mL per minute identifies individuals who are at high risk for CIN.12 It is for these individuals that prophylactic strategies have been developed.
The first step is asking whether the information required for diagnosis of the condition under study can be obtained using a modality that does not use iodinated contrast. For certain conditions, ultrasonography or MRI might be appropriate alternatives. In other cases, noncontrast CT might be sufficient. Obviously, avoidance of iodinated contrast represents a surefire way to prevent CIN.
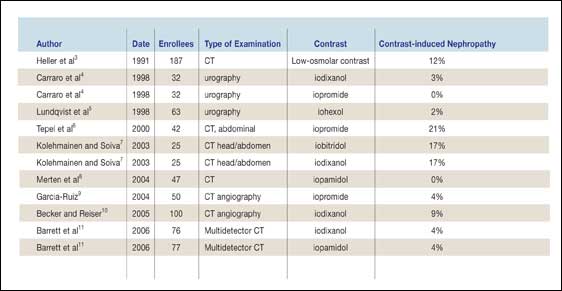 |
| Table. Incidence of contrast-induced nephropathy in patients with renal insufficiency receiving intravenous nonionic contrast (Click the images for a larger version.) |
The next step involves addressing expected decreases in renal blood flow. These decreases may occur as a result of intravascular volume depletion, hypotension, decreases in cardiac output, or shunting of blood away from the kidney. Clinical information will usually reveal these conditions. Since contrast administration results in a further decrease in renal blood flow, leading to ischemic injury in the medulla of the kidney, pre-existing reductions in renal blood flow can be expected to increase the risk of CIN. Decreases in renal blood flow resulting from volume depletion and hypotension may be corrected by IV administration of saline solutions. For some patients, withdrawing loop active diuretics might provide additional support for renal blood flow.
A prospective randomized clinical trial by Mueller compared different protocols for the administration of IV fluids in these high-risk individuals. In general, it is necessary to administer solutions containing sodium chloride, rather than 5% dextrose in water (D5W). When half-normal sodium chloride is used, a longer period of administration (12 hours) at an infusion rate of 1 mL/kg per hour is recommended prior to contrast exposure. For the use of normal saline, the precontrast time can be reduced to 4 hours using the same infusion rate. Bolus administration of normal saline at the time of contrast exposure and aggressive intake of water alone prior to contrast exposure are not protective. This does not mean that restriction of water prior to contrast exposure is a good practice. The risk of CIN is reduced when urine output is increased.14 One way to facilitate diuresis is to encourage patients to drink water liberally the night before the contrast study.
An important part of the pathophysiology of CIN involves the generation, within the kidney, of oxidative stress molecules (reactive oxygen species) as a result of contrast’s effects on tubular cells.15 Alkalization of the urine appears to accelerate the removal of these injurious molecules and/or reduce their generation. The administration of isotonic sodium bicarbonate (three ampules of sodium bicarbonate in 1 L of D5W) has been shown to reduce the incidence of CIN in a small study8 of high-risk patients. The advantage of this therapy is that it was administered for only an hour prior to contrast exposure (infusion rate: 3 mL/kg per hour). All IV fluids are continued for at least 6 hours following contrast exposure at a rate of 1 mL/kg per hour.
Another strategy involves the use of antioxidants (N-acetylcysteine and ascorbic acid). The benefits of N-acetylcysteine were first demonstrated in patients with renal insufficiency who were undergoing abdominal CT studies using a low volume of nonionic contrast media.6 Subsequently, N-acetylcysteine has been extensively studied, though primarily in patients undergoing cardiac catheterization. A number of meta-analyses reviewed in Briguori16 found a beneficial effect, although it did not reach statistical significance. There is great heterogeneity among the studies reflecting different patient populations and dosing regimes for N-acetylcysteine. The most widely used protocols involve oral administration that must be commenced the day before contrast exposure, thus limiting the practical use of this approach for outpatient studies. In addition, the doses used were those described in the original study, involving a low volume of iodinated contrast for CT studies. Patients undergoing cardiac catheterization often receive two to three times as much contrast, which is given intra-arterially. These differences in route of administration and contrast dose may account for the equivocal results. In fact, a recent comparison of double-dose and usual-dose N-acetylcysteine showed a greater reduction in CIN incidence for the double dose.17
Facts about CIN
- Radiocontrast material was administered to more than a million patients in 2003.
- Contrast-induced nephropathy is the third most common cause of in-hospital acute renal failure.
- Risk factors include the presence of other drugs that may adversely affect the kidney:
- nonsteroidal anti-inflammatory drugs
- aminoglycosides
- angiotensin-converting enzyme inhibitors
- angiotensin-receptor blockers
- Risk factors calling for an estimated GFR:
- more than 70 years old
- history of diabetes, renal disease,
- hypertension, cardiac disease
- No current treatment can reverse or ameliorate CIN once it occurs, but prevention is possible.
A great deal of literature has focused on the choice of contrast as a determinant of CIN. First, the volume of contrast administered is a very significant risk factor for CIN. Every effort should be made to minimize the volume of contrast administered, therefore. In the case of CT angiography, a number of studies have demonstrated that saline chases, power injectors, bolus profiling, and careful timing of image acquisition can all reduce the amount of contrast needed for a given study.
Small, prospective randomized studies4,7,18,19 (of around 100 patients) enrolling patients at high risk for CIN and comparing different contrast media have found significant differences in some, but not all, trials. This is true for both the intra-arterial and IV administration of contrast. A meta-regression analysis2 using predefined inclusion criteria collected data from 22 trials involving 3,112 high-risk patients. This analysis found that some contrast media were consistently associated with a higher incidence of CIN. Controlling for the use of antioxidants, the baseline serum creatinine, the presence of diabetes, the subject’s age, and the volume of contrast administered did not change the overall result (see figure).
A different approach to the same question was employed to evaluate spontaneous adverse event reports submitted to the US Food and Drug Administration. Using statistical techniques (disproportionality analysis), the authors2 also found that iohexol was associated with a significantly higher incidence of adverse renal effects. Both of these analytic approaches suggest that when the risk of CIN for different contrast media is considered along with the kinds of patients and procedures seen in everyday clinical practice, real differences among the agents exist. The mechanisms underlying these differences are unclear. The data do not support the concept of osmotoxicity, by which the risk of CIN is explained by the osmolality of the contrast.1 Some other characteristic of the contrast (chemical structure, ionicity, or viscosity) presumably contributes to the nephrotoxicity of these agents, either by enhancing their effects to reduce renal blood flow and/or by increasing the generation of reactive oxygen species.
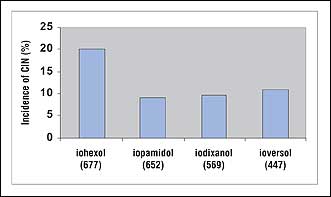 |
| Figure. The unadjusted rate of contrast-induced nephropathy (CIN) for those contrast media to which more than 300 patients were exposed. (Click the images for a larger version.) |
One of the reasons to be aggressive in attempts to reduce the incidence of CIN is that patients who develop this renal complication have higher morbidity, mortality, and use of hospital resources than those who do not develop CIN. Within the coronary catheterization literature,10,16,17 a threefold to fivefold increase in in-hospital mortality has been consistently noted in patients who develop CIN. This holds true for patients undergoing cardiac catheterization, as well as for those undergoing CT studies.22 Mortality may increase to as much as 40% for patients with baseline glomerular filtration rates of less than 30 mL per minute who undergo cardiac diagnostic and interventional procedures.23 Protecting these patients remains a major challenge.
Two studies24,25 (reviewed in detail by Fought) reported a decrease in mortality in these patients when they were treated prior to contrast exposure with 6 hours of hemofiltration. Although these were small studies, the impressive results cannot be ignored, and serious consideration should be given to use of this invasive approach at each institute with a large-volume interventional program.
A number of novel approaches to reducing the risk of CIN are discussed by Fought. All of these strategies rely on assessing changes in renal function through the use of a marker such as serum creatinine. Segal presents a detailed discussion of the pitfalls of using serum creatinine. Understanding of these critical issues is necessary for anyone setting up screening protocols for high-risk patients. Furthermore, they are essential for understanding how CIN is defined and planning how to follow patients after contrast exposure. The practical issues of screening and follow-up are also discussed from the radiology perspective by Ebert.
Richard Solomon, MD, is professor of medicine, University of Vermont College of Medicine, Burlington, and chief of the Renal Division, Fletcher Allen Health Care, Burlington, Vt.
References
- Solomon R. The role of osmolality in the incidence of contrast induced nephropathy: a systematic review of angiographic contrast media in high risk patients. Kidney Int. 2005;68:2256-2263.
- Solomon R, DuMouchel W. Contrast media and nephropathy: findings from systematic analysis and FDA reports of adverse effects. Invest Radiol. 2006. In press.
- Heller CA, Knapp J, Halliday J, O’Connell D, Heller RF. Failure to demonstrate contrast nephrotoxicity. Med J Aust. 1991 Sep 2;155(5):329-32.
- Carraro M, Malalan F, Antonione R, et al. Effects of a dimeric vs a monomeric nonionic contrast medium on renal function in patients with mild to moderate renal insufficiency: a double-blind, randomized clinical trial. Eur Radiol. 1998;8:144-147.
- Lundqvist S, Homberg G, Jakobsson G, et al. Assessment of possible nephrotoxicity from iohexol in patients with normal and impaired renal function. Acad Radiol. 1988;39:362-367.
- Tepel M, Van Der Giet M, Schwarzfeld C, Laufer U, Liermann D, Zidek W. Prevention of radiographic-contrast-agent-induced reductions in renal function by acetylcysteine. N Engl J Med. 2000;343:180-184.
- Kolehmainen H, Soiva M. Comparison of Xenetrix 300 and Visipaque 320 in patients with renal failure. Eur Radiol. 2003;13:B32.
- Merten G, Burgess WP, Gray LV, et al. Prevention of contrast-induced nephropathy with sodium bicarbonate: a randomized controlled trial. JAMA. 2004;291:2328-2334.
- Garcia-Ruiz C, Martinez-Vea A, Sempere T, et al. Low risk of contrast nephropathy in high-risk patients undergoing spiral computed tomography angiography with the contrast medium iopromide and prophylactic oral hydratation. Clin Nephrol. 2004;61:170-176.
- Becker C, Reiser MF. Use of iso-osmolar nonionic dimeric contrast media in multidetector row computed tomography angiography for patients with renal impairment. Invest Radiol. 2005;40:672-675.
- Barrett B, Thomsen H, Katzberg R. Nephrotoxicity of low-osmolar iopamidol vs iso-osmolar iodixanol in renally impaired patients: the IMPACT study. Paper to be presented at: 2006 Annual Meeting of the Radiological Society of North America; November 2006; Chicago.
- McCullough P, Sandberg KA. Epidemiology of contrast-induced nephropathy. Rev Cardiovasc Med. 2003;4(suppl 5):S3-S9.
- Mueller C. Prevention of contrast-induced nephropathy with volume supplementation. Kidney Int Suppl. 2006 Apr;(100):S16-9.
- Stevens M, McCullough PA, Tobin K, et al. A prospective randomized trial of prevention measures in patients at high risk for contrast nephropathy. J Am Coll Cardiol. 1999;33:403-411.
- Persson B, Hansell P, Liss P. Pathophysiology of contrast medium-induced nephropathy. Kidney Int. 2005;68:14-22.
- Briguori C, Marenzi G. Contrast-induced nephropathy: pharmocologic prophylaxis. Kidney Intl. 2006;69: S30-S-38.
- Briguori C, Columbo A, Violante A, et al. Standard vs double dose of N-acetylcysteine to prevent contrast agent associated nephrotoxicity. Eur Heart J. 2004;25:206-211.
- Aspelin P, Aubry P, Fransson S, et al. Nephrotoxic effects in high-risk patients undergoing angiography. N Engl J Med. 2003;348:491-499.
- Chalmers N, Jackson RW. Comparison of iodixanol and iohexol in renal impairment. Br J Radiol. 1999;72:701-703.
- Rihal C, Textor SC, Grill DE, et al. Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation. 2002;105:2259-2264.
- Gruberg L, Mintz GS, Mehran R, et al. The prognostic implications of further renal function deterioration within 48 h of interventional coronary procedures in patients with pre-existent chronic renal insufficiency. J Am Coll Cardiol. 2000;36:1542-1548.
- Levy E, Viscoli CM, Horwitz RI. The effect of acute renal failure on mortality. A cohort analysis. JAMA. 1996;275:1489-1494.
- Marenzi G, Lauri G, Campodonico J, et al. Comparison of two hemofiltration protocols for prevention of contrast-induced nephropathy in high-risk patients. Am J Med. 2006;119:155-162.
- Marenzi G, Marana I, Lauri G, et al. The prevention of radiocontrast-agent-induced nephropathy by hemofiltration. N Engl J Med. 2003;349:1333-1340.

