Interventional, MRI, CT Codes To Take Brunt of Cuts in 2007
The most contested budget bill in recent history narrowly passed the House of Representatives (216-214), and President George W. Bush signed the bill into law February 8. Although a challenge in an Alabama court is attempting to overturn the bill on the basis of a clerical error, beginning in 2007, the Deficit Reduction Act of 2005 calls for the technical component reimbursed under the Medicare Physician Fee Schedule (MPFS) to be paid at the lower rate specified by the two outpatient imaging systems: the Hospital Outpatient Prospective Payment System and the MPFS.
 The data in this table was drawn from the complete tabulations performed by the American College of Radiology. (Click the image for a larger version.) The data in this table was drawn from the complete tabulations performed by the American College of Radiology. (Click the image for a larger version.) |
The American College of Radiology (ACR), Reston, Va, compiled a list of imaging services affected by the caps. The tallies at the top of the table at right, however, do not include the 25% MPFS reduction for 2006. The ACR used the CMS Impact/Utilization file containing data from 2004, then crosswalked it through 2005 and 2006. Using the conversion factor of $37.8975 and multiplying it with the total RVUs, the ACR calculated the physician office payments. Dollarwise, the total impact to MRI codes is the most significant at a reduction of $18,883.46, compared to ultrasound at $968.77. Not all studies will see a reduction because of the cap, such as many of the x-ray studies, fetal ultrasound studies, thyroid imaging, and colon cancer screening. The DRA excludes mammography, and a decision on whether to include PET—classified as a carrier-priced procedure—is pending clarification from Congress.
“We will now work to repeal the imaging provisions of the act,” says James P. Borgstede, chairman of the ACR Board of Chancellors. “We have a coalition of industry, other specialties, and the American Medical Association to work on this effort.”
The complete comparison lists can be accessed at www.acr.org/s_acr/sec.asp?CID=3140&DID=18881 .
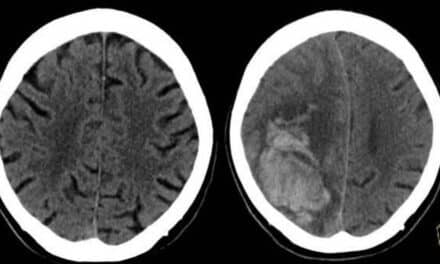
CT Enteroclysis Superior for Detecting Abnormalities in Crohn’s Disease Patients
A study published in the December issue of the American Journal of Roentgenology (AJR) found that a higher percentage of radiographic changes were detected in patients with Crohn’s disease using CT enteroclysis as opposed to conventional enteroclysis, the industry gold standard.
The authors of the study wanted to discover if the newer technique—CT enteroclysis—leads to the same results as conventional enteroclysis. Both methods require a patient to be inserted with a gastric tube—in the conventional method, 300 mL of barium and 1,500 mL methylcellulose solution was combined and flowed through a nasogastric tube placed at the duodenojejunal flexure; in the CT enteroclysis method, 1,500 mL of methylcellulose solution was used via roller pump. CT scans were performed on a single-detector scanner with a collimation of 5 mm, and were analyzed only in the axial plane, according to the authors.
“The CT is more convenient for patients because investigation time is shorter,” says Johannes Sailer, MD, the study’s lead author. “For example, the CT scan takes about 3 minutes, and the whole conventional enteroclysis technique depends on the velocity of the small bowel. The investigation takes at least 20 minutes.”
Fifty patients with histopathologically proven Crohn’s disease participated in the study held at the Medical University of Vienna. Both techniques were successfully done in 100% of the patients. In 88% of the patients, CT enteroclysis found Crohn’s disease-associated radiographic changes, compared to 84% with conventional enteroclysis. Both methods detected stenotic bowel segments in 68% of patients. CT enteroclysis found higher percentages of prestenotic dilatation (40% vs 30%), fistulas (36% vs 16%), skip lesions (34% vs 6%), conglomeration of bowel loops tumors (26% vs 6%), and abscesses (16% vs 0%).
“The definitive benefit of CT enteroclysis in comparison to conventional enteroclysis is that only CT enteroclysis can show the extraintestinal complications of Crohn’s disease,” Sailer says. “With endoscopy, you can just see the last 10 cm of the small bowel when you go into the colon.”
The improved detection comes at a cost though. “CT is more expensive to perform than the conventional enteroclysis,” Sailer says. “Especially when you use a multi-detector CT, it is definitely more expensive than conventional fluoroscopy.”
The authors conclude that CT enteroclysis is superior to the conventional method in detecting abnormalities, and should replace conventional enteroclysis in patients with known Crohn’s disease. They acknowledge, however, that “the diagnostic value of CT enteroclysis has not yet been established in comparison with the current gold standard (ie, conventional enteroclysis) in evaluating small-bowel disease.”
Boston Scientific Swoops In, Buys Guidant
It was the kind of maneuver that gives business observers a warm and fuzzy feeling. When Boston Scientific, Natick, Mass, beat out health care industry giant Johnson & Johnson (J&J), New Brunswick, NJ, in purchasing Guidant Corp, it was more than the little guy winning: It was how they did it.
In December 2004, J&J made a deal with Guidant, Indianapolis, to purchase the company for $76 per share in cash and stock, according to the Wall Street Journal. When Guidant was forced to issue recalls on its defibrillators because of product malfunctions, federal investigations, and patient lawsuits, J&J lowered its offering price to $63 per share in November 2005. Boston Scientific saw an opportunity, and jumped on it.
In December 2005, Boston Scientific made an informal offer to Guidant for $72 per share, which was turned down for the lower J&J offer, according to the Wall Street Journal . The company then offered $73 per share, only to be rejected again for a lower $71 per share offer from J&J.
Then Boston Scientific, with the help of Abbott Laboratories, offered $80 per share in mid January—$4 more than J&J’s original offer. Guidant accepted the offer, over the $71 per share bid from J&J, but gave the company 5 days to make a counteroffer.
In order for J&J to make a competing bid, according to the Wall Street Journal, it would have to have offered at least $77 per share—just $1 more than its original 2004 offer, a psychological barrier the bigger company could not overcome. J&J did not make Guidant another offer.
The little company that could—and did—will now have a combined revenue of about $9 billion, and will hold the No. 1 spot in the United States in selling coronary stents, as well as the No. 2 spot in selling implantable defibrillators, according to the Wall Street Journal.
SCAR To Feature More Exhibits, Futurist Keynoters at 2006 Meeting
This year’s Society for Computer Applications in Radiology (SCAR) Annual Meeting will see more than 130 exhibitors, making this the largest exhibition in its history. “Imaging Informatics in Focus,” to be held April 27-30 in Austin, Tex, will also see two new structural program changes: an “Imaging Informatics” preconference course to be offered on April 26, and a DICOM calibration demonstration on April 28, says Caroline Wilson, director of publications and media for SCAR.
Ben Shneiderman, PhD, professor with the Department of Computer Science at the University of Maryland, will present the keynote address during the opening session to be held on April 27 at the Hilton Austin Hotel. The address, “Leonardo’s laptop: Next generation user interfaces for medical informatics,” will focus on current challenges for medical informatics interface designers to manage the information flow and create a productive method for achieving effective decision-making.
Douglas Lenat, PhD, president and CEO of Cycorp, Austin, Tex, will present the keynote address during the closing session, to be held on April 30 at the Hilton Austin Hotel. His address, “Computers vs common sense,” will focus on the timetable of artificial intelligence, and how those in the digital medical imaging arena will benefit from technologies emerging from this field.
SCAR attendees can expect news on the SCAR TRIP™ Initiative, an update at the R&D Symposium, and a private forum for corporate TRIP partners; an announcement on the SCAR certification program for imaging informatics professionals; and an announcement about where SCAR is heading in the future, Wilson says.
Attendees also are invited to participate in facility tours that are being offered in conjunction with Austin Radiological Association, which owns 15 imaging centers and covers 15 hospitals, and roundtable breakfast discussions will be facilitated on six different topics: residents, PACS administrators, grant funding opportunities, systems architecture, career development, and open source.
For more information on SCAR 2006, or to register, call (703) 757-0054, or visit www.scarnet.org .
Updated MRI White Paper to Help Establish Safety Guidelines
Scissors flying from hands, fire extinguishes going airborne, patient pacemakers or insulin pumps failing: all are safety hazards that MRI facilities must contend with.
According to an article by Mitka in the November 3 issue of the Journal of the American Medical Association, the Food and Drug Administration does not have a standardized policy in place for facilities to report safety accidents, although it does require a facility to report a serious incident—life-threatening or those requiring overnight hospitalization. The article also states that more than half of nonhospital imaging is now performed by nonradiologists who may lack proper safety training.
In response to concern about persistent reports of accidents, the American College of Radiology (ACR), Reston, Va, is updating for the second time the ACR White Paper on Magnetic Resonance Safety produced in 2002 that provides guidelines facilities should adhere to.
Emanuel Kanal, MD, director of magnetic resonance services and professor of radiology and neuroradiology at the University of Pittsburgh Medical Center, lead author of the ACR white paper, and chair of the ACR Committee on MRI Safety, says there are two types of injuries that occur: injuries to patients, and injuries to health care practitioners and others working around the magnet.
He, along with the 14 other members of the ACR Blue Ribbon Panel on MR Safety, authored the 2002 white paper that has quickly become the standard in the field of MRI safety. The authors’ objective was to provide facilities that had no MRI safety policy in place with the guidelines set forth in the document. The basis for the guidelines came from the policies instituted by the University of Pittsburgh Medical Center for its MRI facility. Among the strategies discussed in the November 3 JAMA article are restricting site access for patients, personnel, and equipment; certification and training of MR technologists; and scanning patients with pacemakers and/or cardioverter-defibrillators.
“[The document] was tweaked, updated, modified, and changed,” Kanal says. “Every single aspect, everything contained in those guidelines, is unanimously agreed to by the entire 15-member panel. If even one person disagreed with something, we modified it until we had unanimity in all the outcomes.”
The paper was updated in 2004, and is currently being updated for 2006, he says. Included in the updated version will be new terminology: MR safe, MR unsafe, and MR conditional. MR safe items, under all circumstances, will not have a harmful interaction with anything in an MR environment. MR unsafe items are grossly magnetic, and are clearly attracted to magnetic field gradients. MR conditional means that under certain conditions, items have been tested and found to be safe. These items must be labeled with the precise conditions under which they were tested.
“Although they are not ACR officially recognized standards, it doesn’t seem to make much difference now because apparently by de facto they have become standards in the industry,” Kanal says.
A copy of the white papers can be accessed on the ACR web site at: http://www.acr.org/s_acr/sec.asp?CID=3260&DID=19517 .
Industry News
Vidar Systems Corp , Herndon, Va, released its Clinical Express 3.0 software for mammography in Chicago at RSNA. This software allows prior film-based studies to be digitized and then reviewed alongside new studies on digital mammography workstations… SunGard Availability Services , Wayne, Pa, has signed a strategic alliance with InSiteOne Inc , Wallingford, Conn, to deliver SunGard’s Service for Medical Images, a study management service to store and access digital images from a secure SunGard archive…Customers have ranked Royal Philips Electronics , Andover, Mass, No. 1 for its Medical Systems division in overall service performance, and No. 1 in overall manufacturer satisfaction, in the 2005 IMV ServiceTrak Patient Monitoring Systems survey for the seventh consecutive year… ODS Medical , Mendota Heights, Minn, has signed a partnership with Merry X-Ray Corporation , Tulsa, Okla, to offer ODS’ PACScomm CD/DVD Image Recording Systems… iCAD Inc , Nashua, NH, and Viatronix Inc , Stony Brook, NY, have announced a development and distribution agreement to provide iCAD’s proprietary CAD technology for use with Viatronix’s 3D CT visualization software. In other news, Medicsight PLC , London, and Viatronix have signed a nonexclusive partnership agreement to incorporate Medicsight’s Colon CAD API and LungCAD API into Viatronix’s V3D Medical Imaging Workstations. Viatronix has signed a partnership with Quantitative Imaging , San Bruno, Calif, to integrate QI’s colon CAD enginePolypPoint™ with its V3D Colon Workstation… Toshiba America Medical Systems Inc , Tustin, Calif, has been granted FDA 510(k) clearance for its Infinix VC-i, its newest angiography platform with a large field of view flat panel detector, and technology for vascular examinations and interventional procedures…In November 2005, the shareholders of StorCOMM and Creative Computer Applications Inc approved the merger of the two companies, which formed Aspyra Inc , Calabasas, Calif… InSightec Ltd , Haifa, Israel, has partnered with the American College of Radiology Imaging Network (ACRIN) to enroll patients in a Phase II study assessing how effectively the ExAblate® 2000 technology can destroy cancerous breast tumors… IDX Systems Corp , Burlington, Vt, has received American College of Cardiology-National Cardiovascular Data Registry (ACC-NCDR®) certification for its Imagecast™ for cardiology solution, now owned by General Electric Healthcare , Waukesha, Wis… IBM , Armonk, NY, and i3 Archive Inc, Berwyn, Pa, have launched MyNDMA, a personal health management portal linked directly to i3’s National Digital Medical Archive of digital mammography images and related data… Barco , Kortrijk, Belgium, and ATI Technologies Inc , Markham, Ontario, Canada, have signed an agreement where ATI will provide Barco with access to its FireGL™ hardware and software graphics technology, enabling Barco to optimize ATI’s graphics processors to meet the specific needs of medical imaging applications.
Letter to The Editor
I must take exception to many of the statements by Howard Kessler in his article “Malpractice: The Pennsylvania Experience” in the December issue of Axis Imaging News. He seems to feel that progress has been made in the malpractice crisis in his state, but I feel that what he calls progress is mostly a step backwards.
It is nice that the state subsidizes malpractice policy payments by radiologists, but this does nothing to bring about tort reform. It simply allows the trial lawyers to continue on their merry ways.
His comments on expert witnesses is interesting but one would have hoped that the judges were doing what the new law states previously. In the end, the judge can still deem anyone he chooses to be an “expert.” The problem of expert witnesses is hardly touched.
He then comments on the section of the new law that mandates that hospitals and radiologists must send a letter of apology to patients about unexpected adverse events. He neglects to state if this is confidential information or if this represents an open fishing pond for the lawyers.
I am sure that the trial lawyers are delighted that the same old system is basically unaffected by the new provisions and that they can look forward to more litigation. Where is the cap on pain and suffering and their fees, among other meaningful changes?
Finally, Dr Kessler feels that it is a “nontraditional approach” for radiologists to work closely with legislators and other interested parties to affect malpractice reforms. I think that most radiologists and their state societies have been doing this for eons.
Murray L. Janower, MD, Boca Raton, Fla
People
|
|
 Paul Wilson
Paul Wilson  Ted Nemetz
Ted Nemetz Richard M. Levy , chairman and CEO of Varian Medical Systems Inc, Palo Alto, Calif, retired as CEO in February. The company’s Board of Directors has elected Timothy E. Guertin , Varian’s president and COO, to succeed Levy. Guertin will retain his title of president, and Levy will continue to serve as chairman of the Board of Directors… Paul Wilson has been named CEO of the DMS Health Group, Fargo, ND, and Nat Geissel has been promoted to president of DMS Health Technologies… Ted Nemetz has been named vice president of Toshiba America Medical Systems Inc, Tustin, Calif, Technology Services Business Unit… Kenneth T. Hertz , CMPE, has joined the MGMA Health Care Consulting Group as a senior consultant to assist medical groups with practice analysis, conflict resolution, budgeting, practice development, and strategic planning…Medicsight PLC, London, has promoted Adam Boyse to chief operating officer…EnovateIT, Troy, Mich, has appointed Jerry C. Cirino as its first Advisory Board Member…ASTRO, Fairfax, Va, has hired Emily Wilson as its government relations representative, and Amanda Sarata as its senior policy analyst…The Radiation Therapy Oncology Group, Philadelphia, has appointed Adam P. Dicker , MD, PhD, as the RTOG vice-chair for translational research and chair of the RTOG translational research program committee…Imaging Dynamics Company, Calgary, Canada, has made several appointments to its North American sales and customer support teams: Terry Jarvie , vice president US sales, southern region; Bruce Ashby , vice president US sales, north eastern region; David Haznedl , OEM project manager; and George DeJarnette , director of customer support… Scott Segell has been named vice president, customer delivery of Vocada, Dallas… Bruce Johnson has retired as president and COO of Richardson Electronics Ltd, LaFox, Ill, but will continue as president emeritus and director of the company. Arthur Buckland has been appointed as president, COO, and board member.