
Newer generations of lung CAD systems address workflow and accuracy issues with greater sensitivity, fewer false positives, and integration capabilities.
 |
Lung cancer is the leading cause of cancer death in both men and women in the United States. According to the American Association for Cancer Research, more than 160,000 people die of lung cancer every year.
In 2008, more than 215,000 Americans will be diagnosed with lung cancer, accounting for approximately 15% of all cancer diagnoses. Only about 16% of these will have been caught at an early stage, when the cancer is still localized.
When lung cancer is detected at this early stage, the patient has a 49% 5-year survival rate. At later stages, that rate falls to 15%. Many, therefore, believe that early detection of lung cancer can improve patient outcomes. The American Cancer Society states that “the earlier cancer is found and diagnosed, the more successful the treatment, thus enhancing the survival rate.”
However, because symptoms do not appear until later stages, few physicians know to even look. Lung cancer is frequently noticed while diagnosing other conditions. Subsequently, radiologists read entire chest scans, a process that can add significant time to an already strained workload.
The amount of image data produced for today’s chest CT is overwhelming and requires significant time to look through it all. “The complexity of exams and the amount of image data presented to radiologists are pushing the limits of what can be processed and viewed,” said Thomas Tynes, president and CEO of MeVis Medical Solutions Inc, Pewaukee, Wis. Computer-aided detection (CAD) programs can help.
 |
| OnGuard is available on the PACS reading station with the push of one button. |
“Typically, the radiologist is not looking specifically for lung cancer but the CAD program is, so it’s a good complementary to what the radiologist is doing on a daily basis,” said Kirk Mundy, vice president of marketing for Riverain Medical, Miamisburg, Ohio.
Lung CAD Today
According to Heidi C. Roberts, MD, associate professor of radiology at the University of Toronto/University Health Network in Toronto, there are two types of CAD programs. “Most CAD systems are targeting the detection of lung nodules, but there are also systems that analyze the nodule—shape, volume, and size,” Roberts said. The latter are particularly useful in assessing growth or following a course of treatment.
The systems approved for use in the United States by the FDA have been approved as second readers. “The intent is to increase diagnostic confidence and improve physician efficiency,” Tynes said.
Frank Klein, vice president of medical imaging at Definiens Inc, Morristown, NJ, explains the three paradigms for CAD use. “The most established is as an aid to the reporting physician. The second is as an independent second reader, replacing the human second reader, to confirm the first reader’s findings. The third is as the initial reader, providing good negative predictive value before any human expert has looked at the digital data set.
To get to such an advanced stage, clinicians need to be confident in the software. Lung CAD programs do improve sensitivity of human readers, and there is much literature that supports this. Tynes cites the primary study used to obtain FDA approval of MeVis’ lung CAD. “It showed a 26% reduction in missed actionable lung nodules with a median false rate of two marks per case,” Tynes said.
 |
| Riverain?s Kirk Mundy says more lung cancer is caught on a plain x-ray than CT because of the large number of people taking them for other reasons. |
CAD can spot lung nodules that the human eye can miss, either because their size is too small or their texture blends too well. “Our product is designed to detect those tumors that are actionable and that the human eye might miss,” Mundy said.
Riverain considers actionable tumors to be between 9 mm and 30 mm. “We don’t want them to be so small that they are not of practicable use, and those over 30 millimeters are generally obvious,” Mundy said.
Systems that are used to follow assess nodule treatment over time often feature even greater sensitivity. “In screening cases, nodules less than 5 mm are unlikely to be of clinical significance, and a low sensitivity for such small nodules may be acceptable. On the other hand, any nodule (particularly a new nodule) in an oncologic patient is primarily suggestive of a metastasis and must be detected regardless of its size; therefore, a high sensitivity is required even for small nodules in these patients,” writes Roberts in a study published last year.
Volumetric measurements also are helpful in treatment monitoring, since they are a direct measure of a method’s effectiveness. “By changing an ineffective therapy, you can not only lower the health care costs but also lower patient pain and improve the outcome,” Klein said.
Improving Past Versions
The systems work only if they are used, though, and there have been some challenges to the widespread acceptance of CAD for lung nodule detection. One of the biggest has been the high rate of false positives. “CAD targets the detection of lung nodules, but it can also point to scars and other abnormal structures,” Roberts said.
The time taken to reject these CAD markings can impact workflow, slowing a radiologist down. If there are too many false positives, the radiologist will be less likely to use the system at all. “Radiologists have a limited amount of time for patient data and want a smooth workflow with not too many clicks,” Klein said.
However, newer generations of CAD feature improved algorithms that have significantly reduced the number of false positives. Roberts estimates there are now about two per read.
Mundy notes the most recent version of OnGuard has about 50% fewer false positives than previous versions. “With each pending version, in addition to becoming more sensitive in detecting nodules, we also reduce false positives,” Mundy said.
Another workflow challenge involves integration. How is the software integrated with the imaging system? How is the information delivered to the physician? How is it reported? “Right now, [CAD systems] run on stand-alone workstations. Integration is the little piece that is still missing and why people are not using CAD on a regular basis,” Roberts said.
Implementation on PACS reading stations may result in workflow efficiency and greater use. “It would be better to have a push button or something easily available on any workstation,” Roberts said. Manufacturers are now offering this capability on newer versions.
Even without it, however, the literature still shows an improvement in workflow. Tynes cites one study that found an average 22% reduction in reading time with the use of CAD.
This may help a CAD system pay for itself, which, considering today’s reimbursement, is pretty much how it is. Currently, CAD for lung nodule detection is not reimbursed by Medicare, and there are no specific CPT codes. Third-party insurers reimburse to varying degrees. Codes do exist for treatment-monitoring functions.
“Lung CAD has been approved by the advisory panel of Medicare although it has refused to attach a dollar value to it,” said Klein, who notes that, in order for it to be paid for, any type of detection program has to be mandated by Congress.
Once reimbursement is granted, the market will likely see a jump in sales. “As we’ve seen with mammography CAD, the moment you get reimbursement, there’s an explosion,” Klein said.
Currently, hospitals seeking competitive and marketing advantages find it is still worth it to invest in the systems. According to Klein, lung CAD systems can run between $70,000 and $100,000. CAD systems give boasting rights to the newest technology and can be used in community outreach programs that use x-rays to screen for lung cancer.
 |
| OnGuard is the only chest x-ray CAD product approved by the FDA. |
“We want to find these cancers when they are treatable. A hospital doesn’t need to find hundreds of patients to be a success. Just a few makes a difference because it is of tremendous importance to the patients and their family,” Mundy said.
OnGuard for X-rays
Community outreach programs often use x-ray systems because they are much less expensive than CT and expose the patient to a lower dose of radiation, but they also are an ideal modality in the hospital for use with CAD because so many chest x-rays are taken. “There are 80 million chest x-rays taken every year and not all are susceptible to lung cancer, but more lung cancer is caught on a plain x-ray than CT because of the large number of people taking them for other reasons,” Mundy said.
Riverain, therefore, designed its OnGuard CAD program to work with x-rays. According to Mundy, it is the only chest x-ray CAD product approved by the FDA. The newest version is pending approval now. It features improved sensitivity and fewer false positives.
The system works using state-of-the-art image enhancement, feature extraction, and classification techniques, and is available on the PACS reading station with the push of one button. “When the physician pulls up the patient record, they’ll have the normal x-ray and the CAD-marked image for easy comparison,” Mundy said.
 |
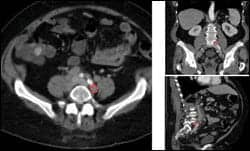
| Definiens is developing a CAD system that will analyze lymph nodes. Show here is the full body segmentation of all organs with lymph nodes (in turquoise). |
Use is easy. “When we demonstrate the product, by the third or fourth image, physicians catch on and know where the CAD program will mark. Logistically, it’s simple, and they can start zipping through images again,” Mundy said. In-service videos also help with on-site training.
MeVis for CT
CT CAD programs work similarly. The R2 ImageChecker from Hologic|R2 was the first system to receive approval from the FDA for use with lung nodule detection. MeVis has acquired the R2 ImageChecker from Hologic|R2 and will reintroduce it as the MeVis Visia CT Lung System this year.
The lung nodule algorithm is advanced and includes a number of criteria for evaluation, including shape, density, size, and anatomical context. Areas of interest are marked for review.
In addition to identifying possible lung nodules, the system offers features that include a temporal comparison tool, which matches and measures candidate nodules on current and prior exams; pulmonary artery analysis, which examines patency in segmental and subsegmental contrast-opacified pulmonary arteries; and automated reporting and PACS integration.
 |
| Only context allows for robust and reliable detection and volumetric quantification of complex structures like lymph nodes, according to CAD developer Definiens. |
The future will likely involve evaluation of lung disease in a broader context. “Most of the CAD products today are focused on lung nodule detection and evaluation of those nodules, but physicians are really interested in looking at obstructive and diffuse disease as well—COPD [chronic obstructive pulmonary disease], emphysema, and fibrosis, as well as better tools for presurgical planning,” said Mundy, who notes the company is looking to provide the most comprehensive CT-based pulmonary imaging product on the market.
Lung CAD for the Future
Other areas for CAD development include other regions of the body. Both Riverain and Definiens are exploring options outside of the lungs. “We are not limited to x-rays or the lungs. We have an active research program that looks at other parts of the body and other diseases,” Mundy said.
Definiens is focused on the electronic analysis of lymph nodes. “Lymph nodes are needed for all cancer staging and restaging, so whenever therapy is assessed and evaluated, people look at lymph nodes. It applies to lung cancer, colon, breast, liver, etc,” Klein said. Because the lymph nodes are small structures scattered throughout the body, a full-body scan is required to see them all, meaning the entire body must be segmented.
Definiens hopes to debut a semiautomatic lymph node CAD in 2009 after 510(k) approval is granted by the FDA, with fully automated detection to follow a year later.
The segmentation technology also can be used for other applications, and the company is currently exploring liver segmentation and head and neck contouring, two regions where technology needs further development. “It’s a very cumbersome job to manually contour the head-neck region, and people can easily spend up to 2 hours to provide this contouring. We have now built the first prototype that does it completely automatically,” Klein said.
The technology is promising, and many expect new CAD programs to mimic the performance of mammography CAD, which has gained broad support and reimbursement although it is not yet a standard of care. As each now generation of CAD system gets smarter, whether detecting lung nodules or breast tumors, it becomes a better tool. If CAD helps to detect any of the more than 215,000 lung cancers expected to be diagnosed in Americans this year at an earlier stage then when they would have otherwise been diagnosed, then it is worth the resources. It can provide a second wind to both radiologists and patients.
Renee Diiulio is a contributing writer for Medical Imaging. For more information, contact .


