When patient Janice Smith was diagnosed with tubular breast carcinoma in 2001 at age 64, she believed that she had one treatment option to save her breast—a lumpectomy with 5 to 7 weeks of radiation therapy—and she was not looking forward to it. But instead, her oncologist introduced her to an FDA- and Medicare-approved accelerated partial breast irradiation (APBI) therapy that treated the lumpectomy cavity in 5 days, not weeks; since then, she has been free of cancer for 6 years.
Smith, who was then a retired hospital data entry worker, had already witnessed the effects of conventional radiation therapy on her husband, who had been treated for lung cancer. She said, “I had been with [my husband] with the external radiation. He had burning of the skin and problems along with that, and I just did not feel like I could do it.”
 |
But when Smith consulted with her new oncologist, she was pleased to learn that she was a candidate for an APBI therapy called MammoSite Targeted Radiation Therapy from Cytyc Corporation, Marlborough, Mass. In addition, she met the selection criteria to become part of a 5-year MammoSite FDA clinical trial.
Conventional whole-breast radiation therapy typically lasts 5 weeks and irradiates the cancerous tissues inside the breast as well as healthy tissues and organs surrounding the breast. MammoSite, however, uses a proprietary balloon catheter that is inserted into the patient’s lumpectomy cavity to deliver a radiation seed into the tumor bed.
In addition to safeguarding healthy tissues, the MammoSite system takes one-fifth the time, lasting only 5 days for a few minutes, twice each day. Six years after her treatment, Smith has had no recurrence of breast cancer, and at age 70, she is working near full-time hours again,
5-Year Results of the FDA Trial
Pamela Benitez, MD, a surgeon at William Beaumont Hospital, Royal Oak, Mich, presented the results of the 5-year trial that Smith participated in at the 8th annual American Society of Breast Surgeons (ASBS) meeting. The results are also published in the October 2007 issue of The American Journal of Surgery.
The 5-year trial followed 43 patients who completed APBI with the MammoSite balloon following lumpectomy and axillary staging.
- Of the original 43 trial patients, 36 have had no recurrence of cancer.
- Seven of the original 43 patients had no recurrence for at least 4 years before having to exit the study because of other conflicting medical conditions.
- Good or excellent aesthetic results occurred in 83% of patients.
- Five-year local recurrence results were similar to those achieved with conventional whole-breast radiation therapy and interstitial catheter brachytherapy.
In addition to the clinical trial, the ASBS has maintained a registry that was initially started by Proxima, the company that originally developed MammoSite’s catheter balloon. Data based from the ASBS registry shows a local cancer recurrence rate of 1.2% at 2- and 3-year points.
Benitez believes that MammoSite is effective because it can focus the radiation directly on the lumpectomy cavity. “The balloon really targets the area of greatest concern,” Benitez said. “Statistically, the local recurrence is most likely going to happen at the tumor bed, so we’re really targeting the radiation therapy to the tissue with greatest risk.”
 |
| Figure 1 |
Lifestyle Advantages to APBI
Benitez has been involved in interstitial brachytherapy research for many years and believes that the MammoSite system gives women better lifestyle advantages over traditional breast-conservation therapy because of its reduced treatment time and convenience.
“There are women who will choose to have a mastectomy because they don’t want to spend 6 or 7 weeks having radiation every day, 5 days a week. There are also women who are afraid of having all that tissue radiated. Then there’s that whole group of women, especially some of the older women, who don’t want to trouble their family members to bring them every day for 6 to 7 weeks,” she said.
Benitez adds that many MammoSite facilities can provide inexpensive local accommodations for women to stay for the 5 days of treatment and then go home.
Smith said that her entire MammoSite procedure was easy and pain free, with none of the burning or other side effects that her husband had. Her only discomfort during the entire 5 days of MammoSite treatment was that she could not take a shower due to the balloon catheter resting inside her breast. Patients are directed not to bathe in order to decrease the risk of infection through the catheter.
 |
| The MammoSite treatment begins with the surgeon first removing the lump. The balloon catheter may be inserted simultaneously or later. |
Patients may also choose conventional interstitial catheter brachytherapy for partial breast irradiation. This therapy uses multiple catheters instead of a single balloon catheter. However, Benitez, who worked with interstitial catheter research in the 1990s, said that this method can be more arduous for both the patient and the physician. She said, “That’s 12 to 18 or more needles across the tumor bed with multiple seeds, multiple drill points, a lot more calculations that have to be done, and a lot more ‘sculpting,’ if you will, of the dose to try to target the lumpectomy cavity. Whereas, with the [MammoSite] balloon, you put it in the lumpectomy cavity, then place one seed into the center of the cavity, and that’s it.”
Kenneth M. Tokita, MD, an oncologist and medical director of the Cancer Center of Irvine, Irvine, Calif, notes that another advantage of APBI therapy over conventional breast conservation is that, unlike whole-breast irradiation, a patient may be treated with MammoSite a second time. He explained, “If a lady gets a second breast cancer in the same breast, almost for sure, she can be treated. In the past, with standard radiation, she really needed to have a mastectomy then, because you can’t [administer] the radiation again to a decent dose. But in this situation, if they get breast cancer again, they can be treated. You just do another lumpectomy and put in a second catheter.”
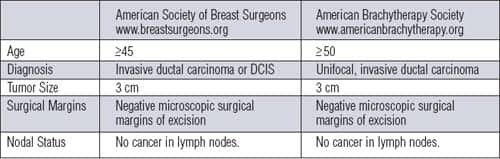
Eligibility Criteria
The ASBS and the American Brachytherapy Society have both established slightly different guidelines for MammoSite Tokita, who also participated in MammoSite’s FDA clinical trial, said that the size limit of a lesion being 3 cm or less does not eliminate many women from the therapy, since most breast cancers are typically no larger than 3 cm.
Aside from clear margins, Tokita said that it is also important to have a reasonable amount of tissue above the cavity in order to avoid having burning near the skin.
“There’s one other [type of breast cancer] that we probably can’t treat,” Tokita cautioned, “and that’s lobular carcinoma. ? The reason for that is that lobular cancer is often multifocal. So, they’re very common in other sites, and if you just treat one, you’re undertreating.”
Tokita also noted that it might now be possible to treat early stage 2 cancers with microscopic disease in one or two nodes, but nothing more invasive than that.
The Treatment
The MammoSite treatment begins with the surgeon first removing the lump. The balloon catheter may be inserted simultaneously, but Tokita said that he prefers that it be inserted later.
“The reason is very simple,” he said. “Number one, the longer the balloon is in there, the higher the risk of infection, which can be a very serious complication. The second reason is that the cost of the balloon is pretty expensive [about $3,000], so you don’t want to put it in there and have to take it out later.”
After surgery, the breast tissue and lymph nodes are analyzed. Also, surgeons assess the cavity size with ultrasound or a CT scan to make sure that it is the appropriate size. If the tissues and cavity size are optimal, then the surgeon can recall the patient in an office visit and insert the catheter into the lumpectomy cavity. In some cases, the surgeon may wish to reconstruct the cavity in order to increase the distance between the cavity and the skin.
Although surgeons may insert the catheter into the original lumpectomy opening, some prefer to create a new incision.
Finally, after the catheter is inserted, the balloon is inflated to the appropriate fill volume, and the insertion point is dressed. The entire process for placing the balloon catheter inside the cavity generally takes about 10 minutes.
After the surgery, the patient reports to the radiation oncologist, who will perform a CT scan to assess the balloon inside the breast for two important factors: One is conformance—making sure that the balloon conforms to the lumpectomy cavity. There should be no air gap or fluid around the balloon, so that the balloon is touching all the breast tissue that needs to be treated. Second, oncologists prefer to have a minimum skin spacing of at least 5 mm, but the ideal is 7 mm or more, in order to protect the skin from any injury.
The last step is calculating the size of the bulb, and then the first radiation seed is inserted into the catheter. Patients receive two treatments per day for 5 days, for a total of 10 treatments. After the last treatment, the catheter is removed in another brief outpatient procedure.
Breast reconstruction is generally not required. “It fills in beautifully,” Tokita said. “The [insertion] tract closes off in about 48 hours, and you don’t even see that anymore.” Likewise, Tokita said that the main cavity normally fills up with fluid within 2 or 3 days after the catheter is removed. Then, over the course of several weeks, the fluid becomes coagulated, allowing scar tissue to grow into the cavity. Generally, one sees very little defect.
Possible Complications
The risk of infection with APBI appears to be similar to whole-breast radiation therapy. In a 2004 paper titled “Partial Breast Irradiation in Breast-Conserving Therapy by Way of Interstitial Brachytherapy” written by Benitez, Chen, et al in The American Journal of Surgery, the researchers compared infection rates in breast cancer surgery with whole-breast radiation therapy to that of surgery with APBI. They found that the infection rates were the same.
Benitez said, “People thought that since you’re doing higher-dose radiation to the tissue you’ll have more problems and more infections. You’ve got these needles traversing the breast tissue and radiating, but actually the incidence of infection was right smack in the middle for what we saw for whole-breast radiation therapy. So that wasn’t any greater with partial-breast radiation therapy than that it was with whole-breast radiation therapy.”
Tokita said that infection can be the most serious complication. “It sounds like nothing because infections are so easy to control nowadays, but in irradiated tissue, infections are very hard for the body to heal,” he said. In a bad case, if the infection becomes uncontrollable, the patient may require a mastectomy to get rid of the infection.
Infections with MammoSite can be caused when the tract for the tube is too tight. When this happens, the cavity will not drain properly, allowing bacteria to get started in the cavity. As an extra precaution, Tokita now uses antibiotics as part of the therapy to further decrease the infection risk.
The Future of APBI
Although the 5-year data is promising, continuing follow-up over the coming years is still needed to determine the long-term efficacy of MammoSite’s APBI technique. Many patients from the original 5-year clinical trial are continuing their participation in the 10-year study.
Tokita is happy with the results of MammoSite thus far and hopes that it will eventually become a more popular alternative to whole breast irradiation. Someday, he hopes to see a time when the 5 days of treatment will be cut down to 1 day, treating the patient with a single dose of radiation. However, he doubts this method will happen in the near term because of the risks associated with such a high dose.
He said, “If you do it all at once, you’re essentially wanting to kill everything that’s in that volume. So, there’s going to be a higher risk of injury and a higher risk of complications, but it will be easier.”
As for Smith, she said she feels healthy since her treatment and is confident that her breast cancer will not be returning. In fact, Smith is pleased to remain a subject in MammoSite’s continuing trials, which will monitor Smith and other MammoSite patients through 10 years after their first treatment.
Tor Valenza is a staff writer for Medical Imaging. For more information, contact .