 |
· Running the Numbers
· Cardiac MRI: Now the Standard for Many Indications
· Study Break: Two recent reports show the power of MRI for
diagnosing ankle pain and MDCT for locating bowel perforation
Running the Numbers
45% of the 26.6 million MRI procedures performed in 2006 used contrast media, according to the 2006 MRI Market Summary Report from IMV, Des Plaines, Ill. The report?which surveyed 7,225 sites about procedure utilization, the MRI installed base and purchase plans, workstations, budgets, and site operations characteristics?found that in 2006, MRI procedures increased 10% from 2003, for an average annualized rate of 3% per year. Compared to 2003, the biggest areas of procedure growth include brain, spine, and MR angiography. Other report findings include:
- 53% of future fixed MRI purchases are planned to be replacements of existing units, 13% first systems, and 34% additional systems;
- 84% of all MRI procedures performed in 2006 were on an outpatient basis, versus 16% inpatient; and
- the average replacement cycle for an MRI is 8.1 years.
Visit www.imvinfo.com or call (847) 297-1404 for additional information.
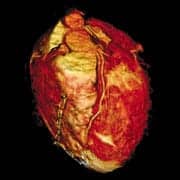
Cardiac MRI: Now the Standard for Many Indications
by Judith Gunn Bronson
The year: 1984. The place: an MRI conference in Texas. The subject: one presenter showed a cin? sequence of the heart that rotated on the screen, displaying the anatomy in spectacular detail. The problem: a great deal of luck had contributed to the capture of the images, and there was no guarantee that the images from the next patient would be as enlightening. Cardiac MRI was in its infancy.
Recent developments have increased the speed, image quality, and reliability of cardiac MRI, and various measures have been implemented to account for or avoid interference by cardiac and ventilatory motion. Thus, MRI’s unique ability to depict both anatomy and function with high temporal and spatial resolution can be exploited. With the most up-to-date scanners and protocols, a study that depicts anatomy, function, blood flow, myocardial stress, and myocardial tissue characteristics can be completed in less than 30 minutes. In 2007, the question about cardiac MRI tends to be only whether expertise for a particular study is available locally, not whether that study can answer a particular clinical question.
The present state of cardiac MRI was reviewed in a November article in Radiology by physicians and engineers from the University of California, Los Angeles, and Siemens Medical Solutions, Malvern, Pa.1 The authors note that although cardiac MRI is still evolving rapidly, it is becoming the standard for many applications.
 |
Comprehensive Anatomic and Functional Imaging
Breath-hold cin? MRI permits combined anatomic and functional imaging to an extent not possible with any other modality. With one protocol, data acquisition can be completed in 20 heartbeats. Temporal resolution has been improved by echo sharing. In an updated protocol, ECG triggering is combined with retrospective gating to further reduce the time required. Ventricular dimensions and myocardial mass can be measured accurately and reproducibly; and ventricular muscle mass, chamber sizes, cardiac output, and ejection fraction can be derived.
In what Finn et al argue is now the standard technique, steady-state free precession (SSFP) protocols with either Cartesian or non-Cartesian sampling are used because of their speed (as fast as 7 seconds) and high contrast-to-noise ratios.1 The differentiation of blood from myocardium is easy, even in patients with poor systolic function. Off-resonance effects that create dark bands on the image are the main drawback, but they can be largely avoided with a highly uniform magnetic field, a large flip angle, and a very short TR (3 milliseconds or less). Speed and coverage can be improved by using some type of parallel imaging, which can acquire multiple sections in the space of a single breath-hold, although there is a penalty in the form of worsened signal-to-noise ratio.
The properties of MRI enable an invaluable technique known as tagging, in which a grid of magnetically saturated tissue is imposed on the heart, and the deformation of the lines is monitored during cin? imaging. Although computer tools are available for quantitative analysis of the deformations, the tools are difficult to use, and it is more common simply to view the sequence of tagged images to identify hypokinetic regions of the heart. Development of this technique, which dates from the early days of cardiac MRI, continues.
An exciting new development is SSFP cin? imaging in real time, which can be performed without cardiac gating or even breath-holding. This method reduces the temporal and spatial resolution but permits studies of patients with severe dysrhythmias. Several protocols are being explored, and the utility of these methods in clinical practice is being defined.
Flow Studies
The phase of an MRI signal can encode information about flow rates, a valuable tool in patients with congenital or valvular heart disease or pulmonary hypertension. Some experimentation with the protocol may be needed, because aliasing may interfere if the flow velocity is high. Finn et al recommend frequent calibration with a flow phantom to avoid inaccuracies in the calculations.1
Postinfarction Evaluation
Another indication for which MRI is standard is assessing myocardial scarring and viability after acute myocardial infarction. The study is considered by many to be superior to nuclear tomography because of its higher spatial resolution. An increase in the permeability of cell membranes in an infarcted area allows gadolinium to escape the blood vessels, causing the contrast agent to accumulate and remain in the affected area. If the correct T1 value is chosen, the infarcted tissue is bright, whereas the signal from the undamaged myocardium is nulled. One caution is that unless there is a long delay between contrast administration and signal acquisition, the scan may overestimate the size of the infarct. Speakers at RSNA 2006 demonstrated the potential of delayed-enhancement studies to predict myocardial recovery.2?6
Techniques for the Future
Efforts to depict the coronary arteries have continued for many years, but the vessels are difficult to capture because of their significant motion with each heartbeat. Current methods are ECG triggered with segmented 3D data capture. A separate breath-hold is required for each of the major arteries, although respiratory gating may be preferable. Like perfusion imaging, vessel imaging is not a routine technique for the heart at present.
To conclude the article, Finn et al note that multidetector array CT is challenging MR in cardiac imaging.1 However, they are confident that MRI will meet the challenge.
Judith Gunn Bronson, MS, is a contributing writer for Medical Imaging. For more information, contact .
References
- Finn JP, Nael K, Deshpande V, Ratib O, Laub G. Cardiac MR imaging: state of the technology. Radiology. 2006;241:338-354. Available at: radiology.rsnajnls.org/cgi/content/abstract/241/2/338. Accessed February 20, 2007.
- Stork A, Lund G, Bansmann M, Muellerleile K, Kemper J, Adam G. Prediction of left ventricular remodeling by infarct size obtained by contrast-enhanced MRI in patients with reperfused acute myocardial infarction [abstract SSK-08-03]. Session presented at: Annual Meeting of the Radiological Society of North America; November 29, 2006; Chicago. Available at: rsna2006.rsna.org/rsna2006/V2006/conference/event_display.cfm?id=66601&em_id=4441604. Accessed February 20, 2007.
- Roes S, Kaandorp T, Bax J, Van der Wall E, Lamb H, De Roos A. Relationship between microvascular obstruction assessed with first-pass perfusion or delayed contrast-enhanced MRI and left ventricular remodeling in patients after acute myocardial infarction [abstract SSK08-04]. Session presented at: Annual Meeting of the Radiological Society of North America; November 29, 2006; Chicago. Available at: rsna2006.rsna.org/rsna2006/V2006/conference/event_display.cfm?id=66601&em_id=4432486. Accessed February 20, 2007.
- Natale L, Meduri A, Bernardini A, Palmucci S, Lombardo A, Bonomo L. The role of no-reflow in left ventricular remodeling after AMI: an MRI evaluation [abstract SSK08-05]. Session presented at: Annual Meeting of the Radiological Society of North America; November 29, 2006; Chicago. Available at: rsna2006.rsna.org/rsna2006/V2006/conference/event_display.cfm?id=66601&em_id=4440477. Accessed February 20, 2007.
- Natale L, Meduri A, Bernardini A, Palmucci S, Lombardo A, Bonomo L. Role of first pass (FP) and delayed enhancement in functional recovery assessment after acute myocardial infarction (AMI) [abstract SSK08-06]. Session presented at: Annual Meeting of the Radiological Society of North America; November 29, 2006; Chicago. Available at: rsna2006.rsna.org/rsna2006/V2006/conference/event_display.cfm?id=66601&em_id=4440408. Accessed February 20, 2007.
- Kaandorp T, Lamb H, Poldermans D, Viergever E, De Roos A, Bax J. Assessment of right ventricular infarction with contrast-enhanced magnetic resonance imaging [abstract SSK08-07]. Session presented at: Annual Meeting of the Radiological Society of North America; November 29, 2006; Chicago. Available at: rsna2006.rsna.org/rsna2006/V2006/conference/event_display.cfm?id=66601&em_id=4440008. Accessed February 20, 2007.
Study Break: Two recent reports show the power of MRI for diagnosing ankle pain and MDCT for locating bowel perforation
A study of 91 patients performed by researchers at Cambridge University Hospitals in England and published in the American Journal of Roentgenology showed that using MR imaging to assess patients with ankle pain changed the course of treatment for 35% of the group.1
Philip W.P. Bearcroft, MD, and his colleagues performed the study in conjunction with an orthopedic foot and ankle surgeon at a regional teaching hospital. “[The 35%] itself is significant, but more significant is the fact that before an MRI was done, 65 of the 91 patients were scheduled to undergo surgery,” Bearcroft noted in a press release. “After an MRI was done, nine of those patients were treated nonsurgically.”
The surgeon noted his proposed treatment plan for each patient before and after an MR examination, along with potential diagnoses for each injury. Before the MRI, the surgeon proposed an average of 2.3 potential diagnoses per patient; this number dropped to 1.2 after the MRI was performed (see Figure 1 below). “This study is a bit different than the traditional radiological study,” Bearcroft observed. “Most studies relate to improving technique or look at the accuracy and predictive value of imaging techniques. This one was designed to determine if we really make a difference to the referring physician and the patient.”
 |
| Figure 1. Changes in diagnostic certainty after MRI for all diagnoses under consideration. Red bars = before MRI; blue bars = after MRI. An entry in the zero column represents postoperative diagnosis of normal. |
Meanwhile, Belgian researchers showed that multidetector CT (MDCT), used without contrast media, can show the precise site of a bowel perforation, circumventing the customary exploratory surgery of a patient’s gastrointestinal tract.
 |
| Figure 2. A 42-year-old man with perforated sigmoid colon diverticulitis. Transverse CT image shows segmental bowel-wall thickening (arrowheads), mild pericolic fat stranding (asterisk), and few extraluminal bubbles of air adjacent to the bowel wall (arrow). Click on image for larger view |
The study,2 also published in AJR, observes that the best method of locating bowel perforation in the past was to administer oral or rectal contrast media and watch to see whether it leaked from the bowel and, if so, where. But lead author Bernard Hainaux, MD, of Centre Hospitalier Universitaire St-Pierre, Brussels, notes that it is difficult to administer contrast media to a patient with acute abdominal pain or penetrating injuries.
According to the study, MDCT without contrast media accurately showed the site of bowel perforation in 73 of 85 patients. Radiologists should be on the lookout for three aspects of the MDCT image: gas bubbles near the bowel wall, a defect in the bowel wall, and thickening of the bowel wall, according to Hainaux (see Figure 2 at right).
“MDCT allows us to quickly image the patient,” Hainaux says, “then reformat the images so that we can look at them from many different angles, making this technique particularly suitable for the assessment of abdominal abnormalities.”
—C. Vasko
References
- Bearcroft PWP, Guy S, Bradley M, Robinson F. MRI of the ankle: effect on diagnostic confidence and patient management. AJR Am J Roentgenol. 2006;187:1327?1331. Available at: www.ajronline.org/cgi/content/abstract/187/5/1327. Accessed February 20, 2007.
- Hainaux B, Agneessens E, Bertinotti R, et al. Accuracy of MDCT in predicting site of gastrointestinal tract perforation. AJR Am J Roentgenol. 2006;187:1179?1183. Available at: www.ajronline.org/cgi/content/abstract/187/5/1179. Accessed February 20, 2007.



