Running the Numbers
Toshiba Installs Beta 256-Slice CT at Johns Hopkins
3T MRI?s First Set of Wheels
ECRI Examines Risks Associated with CT Scans, Publishes Guidance on CT Safety
Running the Numbers
97% of cardiac catheterization lab sites have and use electronic archiving only; 1% use cine film only, and the remaining 2% use both, according to the 2006 Cath Lab Census Database and Market Summary Report from IMV, Des Plaines, Ill. The report?which describes trends in patient cases, cath lab imaging systems, diagnostic review stations, intravascular ultrasound, contrast media utilization, and more?compiles interview data from 1,970 cardiac cath lab sites conducted in 2006. Other report findings include:
- 4.21 million patient cases were performed, representing a 9% increase from 2002;
- 30% of sites have capital budgets of more than $1.5 million;
- 42% of the cath labs have one room, 27% have two rooms, and 31% have three or more rooms; and
- 88% of the cath lab sites have diagnostic-quality digital review stations located outside of their rooms.
Visit www.imvinfo.com or call (847) 297-1404 for additional information.
Toshiba Installs Beta 256-Slice CT at Johns Hopkins
 |
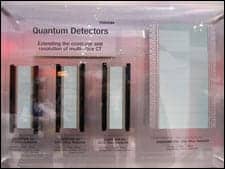
| The prototype 256-slice detector (far right) from Toshiba Medical was on display at the company?s RSNA booth next to its much smaller ancestors, aptly illustrating the exponential leap that the technology represents. |
This month marks the first US installation of a 256-slice CT scanner, and Johns Hopkins University School of Medicine?s Heart Institute, Baltimore, is the beta site, announced Toshiba America Medical Systems, Tustin, Calif, at RSNA 2006. Johns Hopkins will test the system, which is designed to cover the brain or heart in a single rotation, for its value in early assessment of critical radiology and cardiac CT protocols.
Doug Ryan, senior director of Toshiba Medical?s CT business unit, explains that the 256-slice scanner will reduce dosage while producing accurate, high-resolution 3D images. The work-in-progress Aquilion 256 also could enable dynamic multiphase perfusion studies on the brain, heart, and other organs.
In a research and development white paper, Richard Mather, PhD, senior manager of CT clinical science at Toshiba Medical, noted, “Achieving complete coverage of the heart or other organs within a single rotation requires a system capable of covering at least 120 mm of anatomy with no table movement.” This 256-slice prototype covers 128 mm of anatomy with 0.5-mm slices.
But Mather also noted technological challenges impeding the development of the 256-slice scanner: “Without high-quality reconstruction algorithms, cone-beam artifacts could limit the system?s diagnostic capability.” Toshiba Medical is working to limit these artifacts using a modified Feldkamp-based algorithm.
The beta 256-slice CT will be at Johns Hopkins for a limited time to acquire data for further clinical research and product development.
? C. Vasko
3T MRI?s First Set of Wheels
 |
| A view of the inside of the first 3T mobile trailer. |
Philips Medical and Oshkosh Specialty Vehicles partner to offer the first 3T MRI trailer
New at RSNA 2006 was the first mobile 3T MRI trailer, developed by Philips Medical Systems, Andover, Mass, and Oshkosh Specialty Vehicles (OSV), Harvey, Ill, enabling the transportation of advanced MRI technology to remote areas. The mobile MRI combines a newly designed OSV trailer with Philips Medical?s new Achieva 3T
X-series scanner, the latter of which also made its debut at RSNA 2006.
“We considered many things when first looking at this project,” explains Dirk Noel, MR field marketing manager for 3T products at Philips Medical. “System weight, shielding, and coach design were some of the biggest obstacles. Other 3T systems on the market are in excess of 15,000 pounds. Combine that with the weight of the coach, and the system would easily exceed what is doable on America?s highways. The new Achieva 3T X-series is a revolutionary design that solves those weight and shielding problems.”
The X-series features RF shielding built into the unit and a stray field comparable to the 1.5T system; magnet innovations include a 50-cm field of view and 4K zero boil-off technology. The vehicle itself features an all-aluminum welded body structure, a 17-inch twin I-beam chassis, and air-ride suspension, along with an industrial-rated HVAC and chiller system.
“The unique benefit of a mobile 3T scanner is its ability to bring state-of-the-art capabilities to remote areas,” Noel notes. “Mobiles allow those facilities that could not otherwise take advantage of such technology to deliver the best in patient care in an affordable manner. Now, customers in even the most remote parts of the country can do applications like fiber tracking, spectroscopy, and functional MRI.”
The Achieva 3T X-series Mobile is the final addition to the X-series line, which also includes the Achieva XR, a rampable high-field MR system installed first as a 1.5T and upgraded at the customer?s behest?with no exchange of the magnet. (To learn more about the Achieva XR, don?t miss “Emerging Technology” in this issue.) Philips Medical expects the Mobile to be released by this summer. “We are doing some final adjustments and testing, and we anticipate a full market release in Q207,” Noel says. “Pricing will, of course, be higher than a typical 1.5T mobile system, but it will be in line with our customer expectations.” He notes that, just like the fixed units, the mobile system can be customized.
Philips Medical will be taking the Mobile 3T on the road to 11 cities during May and June. To register, visit www.medical.philips.com/goto/mrroadshow.
? C. Vasko
ECRI Examines Risks Associated with CT Scans, Publishes Guidance on CT Safety
 |
By Jason H. Launders, MSc
CT uses x-ray radiation, which is a known carcinogen. However, since the introduction of CT more than 30 years ago, the incidence of cancer within the United States has remained stable while the mortality rate has declined. One of the many reasons for this decline has undoubtedly been the availability of the diagnostic information provided by CT. The precision of today?s radiotherapy treatment planning would be unthinkable without CT. Not only does CT provide high-quality information, but it also is efficient, inexpensive, and noninvasive. As a result, CT has become an essential modern medicine tool, and it?s very hard to imagine health care without it.
In the early days of CT, the long image-acquisition times and limited spatial resolution restricted the number of patients and the quality of diagnostic information. As a result, use of the modality was limited. Most patients referred for CT were diagnosed already or were strongly suspected of having a life-threatening condition.
However, CT technology has evolved rapidly so that now, exam times are much shorter, the cost of the technology has dropped in real terms, and far more detailed information is produced. An analysis of the number of CT scans shows that the use of CT in the United States grew, on average, 9% per year between 1992 and 2002. More recent technological developments, like the ability to scan the heart, means that it can be used for more indications and screen healthy patients. Therefore, the use of CT is likely to grow further. The danger is that as hurdles regulating access to CT drop, the risks associated with the modality will begin to outweigh the benefits.
Risks Associated with CT Radiation Dosage
A number of surveys have shown that medical professionals and patients have a poor understanding of the risks inherent with any CT exam. The chance of a single CT exam with a 10 mSv dose causing cancer seems small (on average, about 1 in 1,000, increasing to 1 in 300 for neonates). But when multiplied by 60 million studies each year in the United States, CT could cause 60,000 additional cancers each year.
However, because most patients will have other health concerns, the actual number of additional cancer deaths is much lower: Estimates are around 2,000 deaths per year in the United States. This discussion highlights two points. First, the risk is much higher for younger patients; and second, the risks of causing cancer are pertinent only if the patient is expected to live long enough to induce the cancer if the CT exam is not conducted. CT is now being used for a much wider patient population, including children, and unless all medical professionals are cognizant of the risks and how to control them, there is a danger that the cancers caused by CT will become a more serious issue.
ECRI Publishes CT Scan Guidance
For more than 35 years, ECRI, Plymouth Meeting, Pa?a nonprofit health care research organization?has dedicated itself to improving patient safety. Its monthly research journal, Health Devices, has long provided recommendations on the safe use of a range of medical devices. In the February 2007 edition of the journal, ECRI addresses issues around the expanding use of CT scans. While the organization believes that CT is an indispensable tool in medicine today, the article cautions that the most appropriate use requires that everyone involved in referring patients to CT, as well as those responsible for the studies, understand the inherent risks and how to mitigate them.
The article discusses the most recent risk estimates for low levels of x-ray radiation made by international bodies and puts them into perspective by comparing them to other sources of radiation commonly used in health care. In addition, the risks of CT use are compared to other well-recognized sources of risk found in hospitals and in our everyday lives.
ECRI also recommends practical ways to reduce the risks, including how to:
- select the right patients;
- communicate with patients;
- adjust scan protocols; and
- use existing dose-control mechanisms.
Because responsibility for the use of CT extends beyond the radiology department, the article is aimed at a general medical audience, not just those directly involved in CT. For more information, visit www.ecri.org.
Jason H. Launders, MSc, is senior project officer (medical physicist) of ECRI, Plymouth Meeting, Pa. For more information, contact .