CAD
Prostate Cancer Tool: A Look at VividLook
With each generation of technology, the tools get better, and with each generation of people, these tools gain greater acceptance. In the medical community, technological advances and adoption occasionally occur simultaneously; at other times, one is ahead of the other. The use of computer-aided detection (CAD) for cancer in medical imaging falls in the first category, with advances and adoption creeping slowly forward together in halting steps.
Acceptance has been hampered by questions regarding CAD’s clinical value in the detection and management of cancer. Yet, ironically, as the technology has improved and come closer to meeting accuracy demands, acceptance has been hindered by a perception of CAD as a threat to personal livelihood and the integrity of the radiology profession as a whole.
CAD, however, is meant to be a tool, not a replacement for the radiologist, and when used properly, it can be a valuable aid in the detection of cancer. Studies have found it can improve accuracy, particularly for inexperienced interpreters. Sohns et al found the use of CAD during mammography reads improved the area under the curve (AUC) of the reading medical student by 10%, the resident by 4%, and a mammography fellow by 3%.1

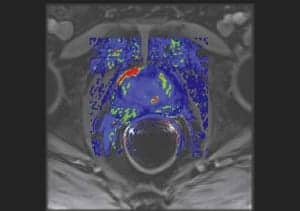
VividLook is a next generation prostate MRI CAD solution from iCAD Inc.
Marc Liebeskind, MD, JD, medical director of New York-based Park Avenue Radiologists, believes there is even greater clinical value in the application of CAD to prostate cancer. “With breast, [CAD] is very helpful, but it’s not dispositive. With prostate, it’s do or die because the gland is a very vascular organ. The way the blood washes in and washes out makes it impossible to detect with the [human] eye. You really do need a mathematical model,” he said.
iCAD AlgorithmVividLook, the next-generation prostate MRI CAD solution from Nashua, NH-based iCAD Inc, incorporates an advanced postprocessing algorithm powered by All-Time Point (ATP) technology to achieve greater accuracy. The ATP analyzes all of the available time points in the dynamic contrast-enhanced MR images in a manner less affected by noise and external factors. The algorithm continuously processes the entire data set against a few discrete time points. Using a pharmacokinetic model to quantitate certain physiological parameters, varying color hues and intensities are applied to help differentiate benign and malignant tumors.
Liebeskind cites better resolution and improved field of view as advantages to the new software. “Particularly with regard to prostate, it’s been able to give me a degree of resolution I haven’t seen in the other products,” Liebeskind said. The performance facilitates interpretation of the more difficult reads typical of patients who have had multiple biopsies resulting in scarring, fibrosis, stones, and other issues that can create an abnormal signal.
An Effective ToolIn his practice, Liebeskind employs CAD in multiple ways, including detection and diagnosis of prostate cancer, lesion follow-up, treatment management, and postoperative care—”we really use it across the board,” Liebeskind says. He sees others adopting CAD MR solutions for prostate in similar fashion.
“[CAD MR solutions for prostate] are maturing really nicely with respect to breast [CAD systems],” he said. Standardization efforts are helping to create greater reliability between prostate scans completed at different centers, enabling easier comparisons. Liebeskind even foresees growth in other organ systems, such as the kidney, liver, and lungs, where analysis of vessel flow through a lesion can help with characterization of disease.
Liebeskind emphasizes the word “help,” stressing that CAD is a tool designed to facilitate radiology workflow but in no way to replace the radiologist. “I think that’s probably the most common misconception about CAD. You can’t look at the image and say it’s red so it’s cancer or it’s blue so it’s benign. It’s part of a thinking process,” Liebeskind said. The fact that interpreter accuracy and improvement with CAD tend to vary with experience bears this out.
As a tool, CAD can improve patient care by enabling radiologists to complete reads more quickly. “Increasingly, we face very high-volume data sets—thousands and thousands of images. So these are really tools to analyze and reduce the amount of information we have to process as individuals so we can then work more clearly,” Liebeskind said.
—Renee Diiulio
Reference
- Sohns C, Angic B, Sossalla S, Konietschke F, Obenauer S. Computer-assisted diagnosis in full-field digital mammography—results in dependence of readers experiences. Breast Journal. July 19, 2010. Available at: www.ncbi.nlm.nih.gov/pubmed/20642459.
CADstream for Liver MRI: Ready, Set, Read
When the first computed-aided detection (CAD) technology came onto the market for mammography, CT, and other x-ray-based applications, the “aid” came in the form of increased sensitivity to potential tumors that might have been missed by a physician.
There’s another meaning to the word “aid” in CAD for MRI applications from Merge Healthcare, Milwaukee, and it comes in the form of increased workflow efficiency.
CAD for breast MR imaging was introduced by Merge in 2002 with its CADstream® Breast MRI application. Since then, the company has developed a CAD application for prostate MRI, and most recently, Merge launched its CADstream Liver MRI application.
As with the breast and prostate applications, the new Merge liver application is designed for increasing workflow efficiency through automating tasks that are essential for diagnosis, but cumbersome and time-consuming for technologists and radiologists.

Recently, Merge Healthcare launched its CADstream Liver MRI application.
Mary Gatewood, director of product management at Merge, said that CADstream’s focus for MRI applications has always been about automating image processing and speeding up workflow, thus helping physicians wade through and manage all of the MR data.
With CADstream for Liver, radiologists still have to review the image sets and identify lesions. However, the time savings are found through a new level of automation. With a few clicks of the mouse, CADstream outlines the lesion area and processes the size and shape, as well as performs 3D image registration.
Gatewood said, “Physicians get over 1,000 images in an MR study that includes a lot of dynamic information—and these are complicated studies. So the idea behind CADstream is to do all of the preprocessing so that when the physician sits down to read the study, it’s ready to read.”
Other features in the program include subtraction images, multiplanar reformatting, and volume segmentation of the entire liver or Couinaud segments and lesion. CADstream also provides tools for a kinetic and diffusion analysis.
Another potential cost-saving feature and confidence builder is CADstream’s motion artifact algorithm. Switched on, CADstream automatically adjusts an image for motion artifact, yet also allows physicians to view the uncorrected version.
Gatewood reports that clients have told her that this motion correction algorithm has often saved patients—and MR technologists—from having to rerun the exam.
Like all CAD software, the CADstream Liver application is fairly straightforward and easy to master within a few hours. Merge can provide either remote training of physicians and technologists, or it can send a Merge technician on-site.
Because the liver MRI application is new, it isn’t currently available with every PACS platform, but Gatewood mentioned that Merge is working on integrating with a number of vendors. Check with your PACS provider or with Merge for availability.
Pricing for CAD Liver application will also depend on your vendor and installations, but should be similar in cost to the other CAD MRI applications.
—Tor Valenza
Making Virtual Colonoscopy Even Better
CT colonography (CTC), commonly referred to as “virtual colonoscopy” takes a great deal of training to read accurately. With thousands of CT image sets to review, even an experienced radiologist can miss a tiny (6 mm) precancerous polyp, risking cancer growth over the next 5 years—or longer—until the next screening exam.
To decrease the risk of missing a polyp further, radiologists can now incorporate VeraLook, a computer-aided detection (CAD) tool from iCAD, based in Nashua, NH.
VeraLook was recently approved by the US Food and Drug Administration (FDA) for virtual colonoscopy applications. In addition to being approved by the FDA, VeraLook can also point to positive results from a new study published in the September edition of Radiology.
The study, “Effect of Computer-aided Detection for CT Colonography in a Multireader, Multicase Trial,” involved 19 radiologists reading 100 CTC exams with and without CAD. The result?—68% (13 of the 19) radiologists had a higher accuracy rate with CAD than without CAD.1
Moreover, for polyps 6 mm or larger, the per-segment, per-patient, and per-polyp sensitivity were all higher compared to non-CAD-assisted readings.
While there was an increase in sensitivity, there was also a slight decrease in specificity. However, overall, the study showed a 6.2% net gain in the number of true positive assessments.
While not intended for primary reads, the Radiology CAD study shows that without any reader assessment, VeraLook “stand-alone” polyp detection was 94.4% sensitive for patients with at least one polyp 10 mm or greater, and 90.2% sensitive for patients with small polyps between 6 and 10 mm.
However, lead author Abraham Dachman, MD, professor of radiology and director of fellowship programs at the University of Chicago, cautions that CAD should be used as a secondary read only.
“CAD is a spell checker,” Dachman said. “Ideally, we’d like the radiologist who’s adequately trained to first read the case and then turn the CAD on and see what it found and if it was something that they missed.”
The extra sensitivity with VeraLook does take extra time. While the CAD product is fairly straightforward and requires minimal training time, the extra CAD step does increase the reading time by a few minutes.
Without CAD, the average interpretation time was 18.8 minutes. With CAD, the readers’ average interpretation time increased by four and a half minutes, and thus the estimated mean interpretation time increased to 23.3 minutes when using the VeraLook software.
However, Dachman noted in an e-mail that these readers had long reading times and were not all experienced with CTC. He commented that experienced readers can usually read a case in about 10 minutes.
Dachman also added that considering the chance that a cancerous polyp will be missed without CAD, the extra four and a half extra minutes are minimal compared with the potential consequences. “In the scheme of how I view things,” said Dachman, “a few minutes are worth it because of the clinical effectiveness. You don’t want to miss any large polyps, because that dismisses a patient as normal who might really be harboring an advanced lesion.”
As for compatibility, iCAD said through a spokesperson that it is in various stages of integration with each of the major players in the CTC review workstation market.
VeraLook will be licensed and sold through iCAD’s various advanced visualization partners, so pricing will depend on the vendor and how it bundles VeraLook with its products. iCAD, however, expects that the pricing will be similar to that of mammography CAD packages.
—Tor Valenza
Reference
- Dachman AH, Obuchowski NA, Hoffmeister JW, et al. Effect of computer-aided detection for CT colonography in a multireader, multicase trial. Radiology. 2010;256(3):827-835.



