
As demand for breast ultrasound screening grows, especially among women with dense breast tissue, one practice implements a smart solution.

Jinnah Phillips, MD, Director of Breast Imaging at Jefferson Radiology.
Sometimes called the Nutmeg State, Connecticut is also known as the Constitution State for its influence over the development of the federal government and the writing of the US Constitution. Over the past several years, Connecticut has taken a significant leadership role in regard to breast density and improving the early detection of breast cancer in women with dense breast tissue.
As the result of efforts from Nancy Cappello, PhD, founder of Are You Dense, Connecticut recently passed two landmark bills. The state became the first to require payors to cover screening breast ultrasound for women with dense breast tissue in 2005, and the first to mandate communication of breast density to patients through mammography reports. According to the legislation, which took effect in October 2009, patient reports must include information about breast density, based on BI-RADS density measurements established by the ACR. If patients are notified their breast tissue is dense, they must also be informed that they could benefit from supplementary screening tests.
As women became aware of the legislation, demand for breast ultrasound screening rapidly outpaced our ability to handle it with handheld ultrasound. The backlog quickly grew to more than 400 patients. Spurred by this demand, Jefferson Radiology, Connecticut’s largest private practice imaging group with 65 radiologists, became the first in the state—and the nation to the best of our knowledge—to create a screening program using Automated Breast Ultrasound.
We installed the somo?v? Automated Breast Ultrasound (ABUS) system from U-Systems in September 2010 and officially began offering ABUS appointments in October. Over the first 3 months of the program, we have averaged 250 ABUS exams a month.
Despite the increased volume enabled by the use of ABUS, our backlog has actually increased since we initiated the screening program. We attribute this to the media attention surrounding the launch. We saw an increase in total patient volume of 15% in November and 10% in December. While some are new patients—as not all local practices are offering screening ultrasound—the majority are existing Jefferson Radiology mammography patients looking to take advantage of this new technology.
Despite improvements in imaging technology, the ability to see small cancers earlier, and the tremendous success in reducing the mortality rate from breast cancer, it often seems that you only hear about mammography and breast imaging when there is a controversy. With this article, I will present a case for proactively adopting new breast imaging technology that improves early detection and patient peace of mind.

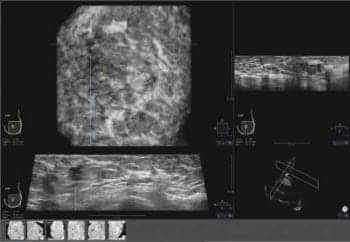
Patient comfort and consistent results are hallmarks of the somo?v? Automated Breast Ultrasound (ABUS) system from U-Systems.
Why Is Density Important?
Breast tissue density not only has been linked to an increased risk of breast cancer, it also decreases the sensitivity of the mammogram. Several studies have confirmed that as tissue density increases, the accuracy of mammography decreases; 35% of breast cancer goes undetected by mammography in women with dense breasts, as density masks the appearance of tumors (Boyd et al, 2007, New England Journal of Medicine). Since both appear white on a mammogram, finding cancers is analogous to looking for a snowball in a snowstorm.
However, it is not all bad news for women with dense breast tissue. Studies confirm that the addition of ultrasound for the screening of breast cancer significantly improves detection rates among women who have dense breast tissue. Data from the ACRIN 6666 Study demonstrated that adding screening ultrasound to routine mammography increased the detection of cancer by 28% over mammography alone.
Handheld Ultrasound vs ABUS
Ultrasound is a proven breast imaging tool that we have used for years for diagnostic purposes and for guiding biopsies and other procedures; however, handheld ultrasound is not well suited for broad screening use. It is operator dependent, with quality highly correlated to experience and training. This can result in variability in perception of lesions, inconsistency in examining the entire breast, and difficulty in consistently confirming inclusion of the entirety of the breast.

The addition of ultrasound screening significantly improves detection rates among women with dense breast tissue.
At Jefferson Radiology, we have a terrific staff of experienced technologists, but many practices do not have the same luxury. As a result, radiologists often feel the need to be present to conduct the handheld ultrasound study. ABUS offers consistent results, and the reduction of operator dependency frees radiologists for more patient visits and other procedures.
The system utilizes a wide field of view, high frequency transducer to acquire large format images, which enable the radiologists to see more breast tissue than conventional ultrasound. The system methodically scans a woman’s breast, capturing up to 350 ultrasound images that can be rendered and reviewed in 3D. This automated approach makes high-volume, cost-effective breast screening possible.
The somosomo?v ABUS system was developed to support the prospective SOMO?INSIGHT Clinical Study. Sponsored by U-Systems, the study is designed to evaluate whether ABUS in combination with digital mammography is more sensitive than a routine screening mammogram alone in detecting breast cancer in women with dense breast tissue. More than 10,000 women have participated in the study, which has identified a significant number of mammographically occult cancers that would not have been detected without the ABUS exam.
Positioning, Positioning, Positioning

Multicystic mass; somo-v? Automated Breast Ultrasound image.
Implementing our somo?v? ABUS breast screening program, we utilized mammography technologists rather than sonographers. Mammography techs understand the nuances of patient positioning as it relates to acquiring reproducible images that can be used to compare temporal changes. Positioning is equally critical to a high-quality ABUS exam, which made cross-training a good clinical and economic decision.
Where handheld ultrasound exams typically take 45 minutes to perform, we’re currently scheduling ABUS exams in 30-minute windows. In reality, our staff can complete a bilateral, full-field breast scan and store the data for review in 15 minutes. Our initial volume of 250 ABUS exams works out to roughly 15 ABUS exams a day. However, we expect to be able to increase this to 30 a day with a single system as we integrate the faster workflow.
Whether we’re figuring a 15- or a 30-minute exam, the ABUS workflow enables us to free rooms more quickly for performing other exams (liver, kidney, etc). It also frees our ultrasound technologists for diagnostic breast and other exams. The result is better resource utilization and revenue opportunities.
Longer Physician Read—Better Diagnostic Confidence
Breast mass; somo-v? Automated Breast Ultrasound image.
In our practice, a normal handheld breast ultrasound will typically be read in 15 to 30 seconds by reviewing key images acquired by the sonographer. With additional images and case complexity, review time for a typical ABUS exam is about 5 minutes. As we gain experience with the ABUS technology, I expect we will be able to bring read times down to 1 to 2 minutes for a normal exam. As with any new procedure, there is a learning curve and we’re dealing with the workflow now.
The trade-off for slightly longer read times is better diagnostic confidence as a result of good image quality and visualization of breast tissue. Like most breast imagers, I believe that my read is only as good as the images I see. With the coronal view capabilities provided by ABUS, I have the ability to interrogate suspicious areas in a 3D plane, offering higher diagnostic confidence. The ability to see the entire breast, not just the samples selected by the technologists, gives you a greater sense of security. With ABUS, you can control the entire review process; you have the ability to look at all of the tissue, to quickly rule out simple cysts and artifacts, and to make more confident decisions. I trust my technologists, but there is nothing like seeing it for yourself to boost your confidence.
ABUS Breast Screening—Forging New Ground
I am proud of the team at Jefferson Radiology for tackling the first-ever large-scale integration of ABUS technology into clinical practice. Creating clinical and operational workflow, we were forging new ground. Generally, this entrepreneurial spirit led to smart, innovative solutions; however, it also resulted in issues with reporting and patient notification. While we didn’t at first, we have now adopted our routine mammography procedures, including the call-back process, the lay letter, and referring physician notifications.
Currently, ABUS exam review is workstation-based. We are working with U-Systems on making ABUS data available throughout the enterprise. Whether you decide to perform daily or batch reads, an enterprise solution would enable exam distribution, resulting in better workflow and faster exam review and reporting.
We do not have definitive reimbursement data yet, but anticipate coverage to be adequate to support the ABUS screening program.
Worthwhile Clinical Addition
Since the Connecticut legislation passed, comparable bills have been initiated in New York, Florida, and Texas with Massachusetts, Missouri, Kansas, and California considering legislation for 2011. On the federal level, the Breast Density and Mammography Reporting Act of 2011 is expected to be introduced by Representatives Steve Israel (D-NY) and Rosa DeLauro (D-Conn).
The national push was bolstered recently as Nancy Brinker, founder and CEO of Susan G. Komen for the Cure, expressed Komen’s position that it should be regular practice for doctors to inform women of their breast density and that it is important for doctors to discuss with their patients with dense breasts what additional screening tools might be appropriate for them.
As concerns regarding breast cancer detection, prevention, and treatment have continued to rise, the forward progress of Automated Breast Ultrasound technology, and the communication surrounding breast density and options for screening women with dense breast tissue, has created a long overdue opportunity for patients and physicians in our state to feel comfortable with breast ultrasound screening by leaving them reassured by the results they receive.
Supported by the fact that we have already identified two mammography occult cancers in the short time that we have been using the ABUS technology, the addition of automated breast ultrasound has significantly expanded our breast imaging capabilities. Being able to offer ABUS for use in combination with mammography for women with dense breasts has been a worthwhile addition to the Jefferson Radiology practice. While there are workflow issues to smooth out, there is no question that ABUS breast screening improves the clinical capabilities of our practice, and I would encourage every breast imaging practice to consider ABUS screening, regardless of the status of density notification laws in their state.
Jinnah Phillips, MD, is Director of Breast Imaging, Jefferson Radiology, which has several offices throughout Connecticut.

