
By L.E. Richey, MD, and Todd R. Richey

Providing diagnostic imaging services is becoming more competitive every day, and increasing economic pressures are some of the most daunting factors in the mix. More expensive equipment, maintenance, repair, and upgrades; steadily increasing labor and material costs; and general overhead coincide with eroding reimbursement as various entities strive to lower the cost of health care. Under these circumstances, imaging centers—especially those that operate independently—must seek out every technological advancement and cost advantage possible to benefit their patients, referring physicians, and the centers themselves. Our job is to be an asset to the referring physicians in treating their patients, but we can only achieve that if we have a healthy balance sheet. In such a competitive environment, we believe that having superior computer-aided detection (CAD) technology is essential.
The Volume Imperative
There was consensus among our physicians and administrators that the major solution to these conditions was a topline one: achieving higher volume. But unlike many businesses that can sacrifice some quality to get volume up, in medicine and certainly in our clinics, reducing quality is not an option. Our adjustments must maintain diagnostic quality and excellent service at the same time that they drive volume—a delicate balancing act. To strike this balance, we need to deploy technologies that achieve more efficient patient throughput while being clinically efficacious. One of the most obvious gains is to cut out the physical transportation of film to an analog CAD processor; sending that data electronically is a certain gain. Further, these technologies must work as seamlessly as possible with one another.
To achieve greater volume while retaining imaging quality, our greatest opportunity came through shifting from analog to digital mammography (DM). It was clear that migrating to digital mammography would be indispensable in driving throughput efficiencies. It was also clear that we had to use a CAD system that would work seamlessly enough with our digital system so that we did not negate the throughput gained by going filmless.
CAD systems can serve as second sets of eyes that enhance readers’ diagnostic confidence. In our case, that confidence helps to speed the process through a significant number of mammography reads every month in our multiple locations—without sacrificing accuracy. But our previous CAD system had the potential to short circuit these gains with false positives, system glitches, and displays that could be difficult to interpret. Indeed, we could not have achieved higher volumes responsibly had we not turned to a CAD system that was significantly better than what we had in every respect.
From Analog to Digital Mammography, Identifying the CAD
As our multiple imaging centers were making the journey from analog to digital mammography, our radiologists devoted a fair amount of time and research to identify CAD systems that would prove clinically effective and work efficiently with our DM and PACS systems. Over the last decade, we had used CAD with film screen mammography, and our experience comported with the general wisdom about the pros and cons of such systems. (The subject of controversy, CAD technology has come under fire in studies questioning its effectiveness.) However, we were encouraged by a new CAD technology introduced by VuCOMP, and we had an opportunity to experiment with it. In addition to having an early look at how it worked, we were encouraged by a new, comprehensive reader study of the same technology: the FDA study has shown that, for the first time, this new approach to CAD leads to improvements in radiologists’ sensitivity to breast cancer as well as in their ability to differentiate between breast cancer and noncancer. As we conducted our own research evaluating CAD systems, we began to understand that this new approach revolved around algorithms that compared multiple images before producing a CAD image with marks, and that it provided greater sensitivity and specificity.
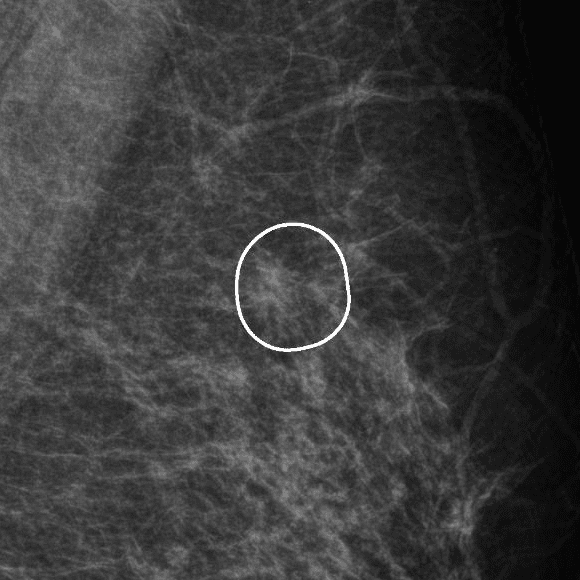 Example of VuCOMP mass detection.
Example of VuCOMP mass detection.
The New CAD Technology in Brief
The technological approach that is yielding the best result in CAD is decision technology, which is oriented toward the most suspicious types of visual structures that appear in mammograms. With this, developers can construct mathematical formulas that represent the concepts underlying these structures—but which also map closely to natural human understanding. The automated intelligence carries out its reasoning in a way that an engineer can interpret more intuitively, which enables engineers to locate and fix problems more quickly. Prior to this innovative approach, CAD systems relied upon “black-box” learning technologies, of which neural networks are examples. Working through a large number of examples, these networks “learn” about a problem, encode the data from these examples, and come up with a set of numbers. While certainly useful in many scenarios, this approach makes it extremely difficult for a human to grasp—and therefore evaluate—what exactly the black box has “learned.”
Now CAD systems can achieve a greater reliability and better performance for our clinics than older systems, which were based on more obscure reasoning.
Significant Impact on Mammography Reader Studies
In short, we are getting better resolution and significantly lower false-positive and false-negative rates with this new CAD system, making our radiologists more effective and efficient. These gains contribute a great deal to our throughput for several reasons, including:
Lower False Positives, Correct Call-Back Percentages
One of the advantage of VuCOMP’s CAD is that, in accordance with our accreditation bodies, it allow us to keep the correct call-back percentages so that we don’t have too many false positives in our mammography program. Combining this new call-back accuracy with CR mammography allows us to increase our throughput dramatically because we don’t have to handle wet film processing.
Seamless Workflow
The reason the CAD system interface is so important is that our techs have to be able to process the study through the system seamlessly. Mammography studies can be held up by processing complexities such as transferring CAD images into the PACS systems and readying them for the radiologist to read. Since its implementation in our clinics, there have been no such integration issues with our new CAD system.
Rapid Processing
Without a CAD that can keep up with the rest of our increased throughput with digital equipment, our gains in speed and throughput would be lost. It is important that the back end of the CAD system quickly process the image to keep up with workflow demands. It must accommodate our needs as fast as any other piece of equipment we have.
Diagnostic Confidence
Complete diagnostic confidence is the radiologist’s holy grail. No matter how many studies we perform in the center, our job is not done until the interpretation is complete and a report has been generated. If there were an inordinate number of false positives and/or false negatives stemming from CAD—or even if the radiologists simply felt no added confidence with the system—it would slow our process down. The advanced product from VuCOMP is living up to the reader study results: it does not return the high number of false positives and false negatives that have held CAD back in the past.
Conclusion
Our experience confirms that realizing the full benefits of digital mammography depends on the integration of a dependable diagnostic CAD system. VuCOMP’s CAD is proving to be a reliable and valuable tool, which aids us in providing highly dependable diagnostic results with increased throughput. This benefits both our own business and the patients and physicians we serve, and allows us some measure of advantage in an increasingly competitive industry, which is forever facing the pressure of declining reimbursements.
####
Tools for the Times
Radiologists are facing growing pressure to handle higher work volumes, and they need tools to cope with this workload increase. This phenomenon is being driven by several factors:
- a shortage of radiologists caused by a decrease in resident programs as well as an increase in subspecialty training (both of which have lowered the supply of general diagnostic radiologists)
- downward pressure on reimbursement, reducing margins and forcing clinics to see more patients
- better technology, which drives imaging services demand and increases throughput efficiency
- a growth in the national population (expected to increase by 16% by 2020), and in particular a projected 50% increase in the 65-and-older age group, which consumes more preventative medicine than previous generations
The relentless challenge to radiologists to accomplish more with less will require more efficient and cost-effective diagnostic and imaging technologies. Radiologists will need to identify the smallest possible anomalies at every opportunity, facilitating the earliest possible therapies. VuCOMP’s M-Vu CAD and other advanced imaging technologies will become ever more important in aiding them.
— L.E. Richey, MD, & T.R. Richey
(Source: LocumTenens.com)
L.E. Richey, MD, is a radiologist, and Chairman and Medical Director of U.S. Imaging, Inc. Todd R. Richey is President and CEO, U.S. Imaging, Inc.
The authors own and operate imaging, sleep, and surgery centers in Texas. In business for 24 years, they currently have 10 outpatient imaging centers in the state. The company is privately held and family owned.

