 |
· Interview with an Inventor
· Tech Zoom: Researchers Examine Fe8 as MR Contrast Agent
· Is 64-Slice Really Better? KLAS Report Weighs Industry Input
Interview with an Inventor
by Renee DiIulio
Joseph P. Culver, PhD, discusses diffuse optical tomography with Medical Imaging
Thanks to advanced imaging modalities, physicians routinely look inside the brain, but many views are limited to a peek?images that indicate what is happening in the brain at that moment. But there are many patients for whom continuous monitoring could bring benefit. Researchers at Washington University in St Louis are at work on a technology called diffuse optical tomography (DOT), which will permit this function.
With seed money from Allied Minds, Quincy, Mass, the two organizations created Cephalogics, Quincy, which will focus on the commercialization of this technology. Medical Imaging spoke with Joseph P. Culver, PhD, assistant professor of radiology at Washington University and the technology’s inventor, about DOT, how it works, what it does, and how it will benefit medicine.
MI: How does diffuse optical tomography work?
Culver: DOT is a computational imaging approach to performing near-infrared (NIR) spectroscopy. It’s based on principles similar to pulse oximetry. The basic idea is to send light through tissue. Oxyhemoglobin and deoxyhemoglobin are the dominant absorbers, exhibiting different NIR absorption spectra in blood.
With pulse oximetry, a lead is placed on one side of the finger and detectors on the other to measure resulting light transmission through the finger. We’re applying these same principles to the brain.
Traditionally, it’s been challenging to get light into and out of the brain. By placing leads every 3 cm externally on a patient’s head, the light transmission from the source gets deep enough to report what is happening in the patient’s brain.
MI: How does the technique differ from other brain-imaging modalities, such as MRI? What advantages and disadvantages exist in comparison?
Culver: DOT potentially fills a functional gap in the neurologic imaging suite of modalities available now. There are the fixed central facilities scanners such as MRI, PET, and CT, and continuous monitoring measures such as intercranial pressures and electric activity (EEG).
DOT provides continuous bedside imaging, is portable, and can be brought bedside. It’s nonionizing, so it does not have the radiation concerns of PET or CT. And it reports brain function with measures of hemodynamics and metabolism, which differentiate it from ultrasound and CT.
MI: In what format are the images produced?
Culver: Everything is digital. The file is more similar to video than a snapshot. Currently, we capture about 10 megabytes a minute, but the work is in the early stages and that number could go up or down. Storage of the files will also evolve.
MI: Who reads the images?
Culver: It would depend on the situation, whether the radiologist or appropriate physician did the reading. The technology is a little bit like EEG or ultrasound, where some of the readings are not necessarily performed by radiologists.
MI: What type of data can be collected?
Culver: Depending on how much light is attenuated at different wavelengths, we can record blood volume and oxygenation in the brain. With the high-performance DOT system, we have improved reliability and imaging resolution, and we are now figuring out where this newer system will have applications.
MI: Cephalogics has stated that an early goal is to develop the system for use with neonates and infants. Why start with neonatal patients?
Culver: Premature infants are particularly vulnerable to brain-related disabilities. The survival rates of preterm infants have improved dramatically, but the long-term developmental outcomes leave a lot of room for improvement. Early detection of alterations in normal brain development or problems with the brain is important for treating and caring for preterm infants. If we can get a functional assessment during the initial hospital stay, it could inform better treatment during a stay or better therapy after the patient leaves.
MI: For which diagnoses and types of patients do you envision the technology’s eventual use?
Culver: There is potentially a wide application. We would like DOT to become the brain equivalent of the pulse oximeter, which is used routinely in the hospital to assess patient status during a number of procedures. DOT could be used to monitor patients with head injuries or stroke or those undergoing procedures such as pulmonary bypass.
MI: Is there a timeline for your progress?
Culver: We’re developing a prototype and aim to have it completed in about a year. We’ll begin pilot studies after that.
Renee DiIulio is a contributing writer for Medical Imaging. For more information, contact .

Researchers Examine Fe8 as MR Contrast Agent
Early research shows promise
MR imaging is good, but it could always be better. Researchers are constantly at work on new technologies to achieve clearer resolution or better contrast. Scientists at Florida State University (FSU), Tallahassee, the University of Colorado, Denver, and the National Institute of Standards and Technology (NIST), Gaithersburg, Md, are collaborating on research into the molecular magnet Fe8 as a contrast agent for MRI. Though in its early stages, the work shows great promise.
Fe8 is a molecule comprised of eight iron ions, which form a tight molecular bond. “Fe8 is a fairly well-characterized material that has a magnetic field three times stronger per molecule than that of the gadolinium compounds frequently used today,” said Naresh Dalal, PhD, the Dirac professor of chemistry and biochemistry at FSU and one of the lead researchers.
 |
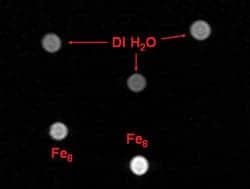
| Molecular nanomagnets create concentration-dependent contrast in MRI. Here they have been used to alter the nuclear properties of hydrogen in water. Courtesy of NIST. |
Because MRI contrast depends on the strength of the magnetic field produced by the contrast agent, Fe8’s stronger field could result in greater contrast, clearer images, and more accurate diagnoses. Currently, the material has been examined using 1 Tesla MR machines, but Dalal expects that the molecule would work as a contrast agent at any magnetic strength. “The stronger field may even be an advantage,” said Dalal.
The material would work in the same way as current contrast agents, through dissolution in water or a medical buffer followed by injection into the patient. Because it is water-soluble, nontoxic, and expected to work at low concentrations, it is also anticipated that Fe8 will produce few side effects. “Iron is present in the body so Fe8 should, in principle, be less toxic than current contrast agents. It can be assimilated by the body whereas gadolinium, for instance, has to be excreted,” said Dalal.
Of course, more research will be needed before the material is developed and commercialized as a contrast agent for MRI. “One of our challenges is to change the compound’s chemical structure using different ligands to make it more stable in aqueous solution,” said Dalal, noting that it is not yet stable enough to ship or store at this stage. The compound breaks down within water in just a few hours.
Fe8, however, is easy to synthesize. “There are no technical difficulties in its synthesis?any organic chemist could produce the compound,” said Dalal, who estimates it takes about a week to make 5 g.
Currently, the work has been done in vitro only; no animal or human trials have been conducted nor has a timeline been solidified. The most recent paper was published in the January issue of Polyhedron and titled “Efficacy of the Single-Molecule Magnet Fe8 for Magnetic Resonance Imaging Contrast Agent Over a Broad Range of Concentration.”
Because the work is so new, it is difficult to project what the clinical applications for Fe8 might be. “We are at a very early stage right now and have not yet worked out the material’s applications or side effects. But we are working hard and may have some more answers within a year or two,” said Dalal.
?R. DiIulio
Is 64-Slice Really Better? KLAS Report Weighs Industry Input
by Dana Hinesly
In its first report on 64-slice CT systems, KLAS, a research and consulting firm based in Orem, Utah, explored how the new, multislice systems measure up for imaging centers and departments around the country.
The inaugural KLAS “64-Slice CT 2007” compiles insights from 130 individuals representing 112 unique organizations. Based on comprehensive interviews, the document takes a closer look at how the modality performs in abdominal/pelvic colonography and full-body, head, spine, chest, CTA, and CCTA scans.
The review includes user comments that were provided during interviews. For many, these observations provide the most valuable insight into how specific systems actually fit into the operational structure of a department.
“A facility can look at the report in several different ways,” said Jeff Boag, director of medical equipment research for KLAS. “A lot of the facilities focus on the qualitative section of our report?reading the overall comments and feedback about the products and the vendor?and that is allowing them to conduct an extra layer of due diligence with a short list of vendors.” For example, many survey participants strongly suggested that site visits be directed by the customer, not the vendor. “The respondents in the study stressed that if you are a freestanding imaging center, you need to go to other freestanding centers and look at their experience with that vendor and product,” he said.
Based on 40 performance indicators, Toshiba America Medical Systems came in at 91.7, GE Healthcare at 88.9, Siemens Medical Solutions scored 88.1, and Philips Medical Systems received an 87.6. All rankings are out of a possible 100. The average score for all 64-slice CT vendor products is 89.0, as compared to the average for all CTs (87.2).
On the surface, there is no great discrepancy between vendor scores, but the comments of survey participants demonstrate definite differences in performance and customer satisfaction.
“Although it is a tight, high-scoring group overall, there are still certain areas where there is deviation between the scores,” said Chris O’Neal, research manager for medical equipment. “I am sure that they are going to want to get as much detailed information as possible, because these systems cost $1.5 million, plus $12,000 a month in maintenance costs?and [facilities] must figure out what is important to them and what they can live with.”
An illustration of this point is downtime. In a high-volume facility, a 64-slice scanner can generate more than $75,000 in revenues each day. Even 2 days of inactivity could cost the facility $150,000.
“So, although the scores are very tight, the providers must do a very good job in the due diligence to make sure they’re selecting the right vendor and the right service contract, because this is a very significant investment for any provider to take on,” Boag said.
The variations between the vendors become apparent upon examining the fine details. When participants were asked to rate all functional strength areas?in addition to downtime, topics included usability and ease of use as well as parts availability?30% of respondents reported missing functionality in their CT solution.
It is important to note, however, that this figure comes from the total responses and that, when looking at individual vendors, KLAS discovered that only 10% of Siemens’ clients reported missing functionality, whereas 50% of Toshiba’s clients reported missing functionality.
“KLAS focuses exclusively on the end-user performance, and in this case, we talked with everyone from CEOs to chief technologists [to find out] about their experience with the vendor and the modality,” said Boag. The study was motivated, in part, by a sampling of freestanding imaging centers that had or were planning to offer cardiac services. “Of those imaging centers, 60% responded that they were going to invest in 64-slice CT, and that was one of the factors that pushed this forward, so providers can really see the performance levels of the different vendors in the space,” he said.
Dana Hinesly is a contributing writer for Medical Imaging. For more information, contact .
Note: The data used in the compilation of this story are from the “64-Slice CT 2007,” published in April 2007, and have been reprinted with permission.


