
Network Infrastructure Costs
Flexible Platform to Enable Interoperability Among 400-Plus Sites
Toward a Paperless Environment
Alliance Aims to Transform Data Into Actionable Information
Network Infrastructure Costs
Five things to know before you plug in
By Dana Hinesly
Whether it is a PACS, RIS, HIS, or other medical-imaging acronym (including MRI, CT, and PET), nothing works without a network. To oversimplify the issue, the network is what all systems, computers, and modalities plug into to be able to speak to each other. In other words, the network is comprised of the switches and servers that power and communicate with machines, all while acquiring, moving, and storing data.
 |
Professionals in well-established or large health care organizations usually do not have to pay this part of the imaging equation much thought. An in-house IT department oversees all of the components to ensure that they run smoothly. But for start-up and independent imaging centers, the responsibility of being “lead techie” could fall to the radiologist or office manager. In that case, keep a few things in mind before getting started.
1) Know How Much You Can Spend
Regardless of whether a facility has been humming along for years or is counting down to its groundbreaking, it is all about the bottom line. The first step is to clearly outline the type of business that will be conducted and what tasks are associated with that.
“The clinical services plan comes first. This plan defines what the business is doing for its customers. Then, the network is built to support that business,” says John Romlein, managing partner of Qualiteering Labs LLP, Thurmont, Md. “You then define the technical support patterns of those clinical services. The equipment plan is overlaid on top of the clinical services plan. Then, you figure out what all gets networked, and that’s really where the network design comes from.”
Exactly how much should be budgeted for a new network? It depends on exactly which components are involved; the price can range from $50,000 to $250,000. This price tag includes a multitude of factors. First, how many floors are occupied? Technology hubs must be placed on every floor, increasing the hardware costs. Also, what types of images are being sent to the server? Digital mammography machines are now gobbling up a gigabit of Ethernet speed.
Answers to these questions come from both the clinical services plan and the vendors providing equipment and systems.
“The fact of the matter is, you just need to install what the PACS vendor is recommending be installed,” says Tim Stampp, CEO of Medical Imaging Specialists, Metairie, La. Along with the manufacturers of other modalities, the PACS vendor will be able to give guidance to the team involved in the process. “I sit down with the vendor, the techs, and the equipment providers,” Stampp says, “and I know where I’m going to put all my computers for my staff.”
Whatever dollar amount is decided on, it is important to remember that “it always goes back to that clinical services plan. What do you need to do so that you can support your plan?” Romlein asks. “Everything must have the goal of supporting clinical operations.”
2) Be Aware of Who Needs to Share Information
Alongside knowing what types of services you are going to provide, you must know who will be receiving them. What is happening with images after they are acquired? If they are being accessed by radiologists remotely, is the system capable of allowing several physicians to simultaneously access the massive files?
“It’s important to make sure you have enough bandwidth coming into the building so that if you have radiologists who are going to be reading from the outside and they want to pull images—or you want to push images to multiple locations—there is enough ‘pipe size’ to get that stuff out,” says Stampp, who advises making the most of partnerships. Locations going only point-to-point—such as from an imaging center to a hospital—should consider other options like a wide area network (WAN). “If an imaging center is a joint venture with the hospital that is 5 miles away, and if the hospital has all of the network infrastructure, all you need to do is get that data to the hospital,” Stampp notes. “Then, radiologists can push and pull it wherever they want it to go.”
As in the civilian world, the ability to transmit files and data via the Web relies on the groundwork laid by local Internet service providers (ISPs). This cost will be factored into the total bill, but otherwise is fairly straightforward. The biggest decision will be exactly how much bandwidth will be provided—and that will be guided by the clinical services plan (and the definition of what services will be provided to whom).
3) Keep Your Cool
Not only is this just generally good advice, it is imperative when dealing with computer systems. Networks are comprised of electrical parts: servers, switches, cables, and wire. In any business organization, they are housed nicely in an oversized, ice-cold closet—affectionately known as either a communications or computer closet.
“Believe it or not, and as silly as it may sound, [air conditioning] is one of the most important decisions you’re going to make,” Stampp notes. “You have to make sure that you have a separate controller for the HVAC [heating, ventilating, and air conditioning] system, so that you can climate control that room. That computer room must stay cold, because you’re going to put your servers, your racks, and your telephone system in there. Don’t be afraid to spend the extra money on the HVAC system.”
4) Learn From the Past
In short, have a disaster plan in place. Although it was not the worst of what happened as a result of Hurricane Katrina, the fact remains that more than one hospital lost every stored image, record, and file—because they were stored in a basement that flooded.
Because of the portability of electronic data, most digital imaging centers store their patient history off-site. There are two basic options for doing this. One is to find a separate physical location from the main server and set up a mirror server capable of working as a backup.
“You should have a disaster recovery plan, a failover plan, and an emergency operations plan—those are HIPAA requirements—and to do that, you need two places to store and operate your electronic systems,” Romlein says. “The idea that you can get by with one data center is a mistake in this day and age.
“Your network obviously would need to connect those two data centers,” Romlein continues. “So, when you’re planning your networks, you should not plan for a single data center concept, but rather for a dual data center concept.”
The other solution is to hire a third-party company to store the data for you. If you go with a third party, Stampp says, “You pay for that service—so don’t forget to think about it and budget for it. [Either way,] someone has to take that data and store it away in case a catastrophe hits the building.”
5) Prepare for Everything Ahead
Preparing for the future also means planning for growth.
“As time goes on, we are always networking more, never less. Your switches need to be upgradeable, and you need to be able to partition the switch both physically and logically,” Romlein advises.
Dividing the hardware so it has the ability to act as two separate pieces of equipment can be beneficial when managing different types of equipment. For example, updates sent to PCs often cause imaging equipment to misbehave. Partitioning the server so that all medical equipment is on one network and all PCs are on another allows for them to be managed differently. “The ability to partition your network for management purposes is one of the big things you need on your checklists,” he says. “As you grow, you want more sophisticated management methods.”
Dana Hinesly is a contributing writer for Axis Imaging News. For more information, contact .
Flexible Platform to Enable Interoperability Among 400-Plus Sites
It is difficult enough to learn the ins and outs of PACS and RIS. But as interoperability between clinical areas and locations increasingly becomes an imperative for hospitals and health care systems, should radiologists need to learn a new user interface associated with a homogeneous information system in order to electronically access a patient’s complete data set? The powers that be at the University of Pittsburgh Medical Center (UPMC) are quite literally banking on the hope that such an overhaul will not be necessary. UPMC recently announced an $84 million initiative to create an information infrastructure for interoperability connecting its 19 hospitals and 400 outpatient sites and doctors’ offices.
 |
The platform for the system will be provided by dbMotion, Raanana, Israel; UPMC, one of dbMotion’s first US clients, will pay dbMotion $35 million to start, including an investment in the company. UPMC anticipates the total cost of implementation, including payment for dbMotion’s services, will come to $58 million.
“We currently have a heterogeneous IT environment,” explains Duane Falk, UPMC information services vice president. “UPMC provides a broad set of clinical services, and what we’ve come to realize is that there’s no single computer system that can meet all the specialty needs for all of those areas. We expect to continue all applications that have been installed and are providing solid value to the clinicians in their areas. We don’t expect to replace those systems. What we’re looking to do is make it easier for the physicians who use those systems to get the integrated data set from across all those different areas.”
Jay Srini is UPMC’s vice president of emerging technologies; as she sees it, the issue of creating an interoperable health care network comes down to best-of-breed versus one homogeneous system for all. “If you look at the market, you’re going to find that new players are coming out with niche products in certain areas of expertise,” Srini explains. “In terms of trying to get everyone onto the best information system, it’s an ever-changing environment. The idea of taking all those pieces and trying to conform them into one system is going to be very expensive.”
Instead, dbMotion will create an architecture that unites all of the individual departments’ information systems, the centerpiece of which will be a consolidated data pool. “Let’s say we need to integrate data across 10 different systems,” Falk says. “The systems remain as they are today, but they will feed key information to the dbMotion clinical data repository. Then, when a user is accessing a patient in the system, that system will get a view of that data for that patient from dbMotion, which will be presented and viewed as a screen within the user’s normal system. Users won’t have to go to another computer system to log in. They won’t have to learn another application. We’ll present the data to users within their customary application.”
Quite an undertaking—but Peter van der Grinten, dbMotion’s general manager for the United States and Canada, maintains that the dbMotion architecture is a far more elegant solution than bringing every department onto a homogeneous information system. (And it is cheaper.) “This is much less expensive, much less intrusive. It doesn’t require the users to learn massive new systems, new procedures, and new policies. It’s not a massive revolution that has to take place where everyone has to convert, where everyone has to have billions of meetings agreeing on every single minute detail. There’s a lot of work to be done, and that’s what the cost represents, but this can evolve over time.”
So, UPMC’s radiologists have nothing to fear from the evolution of the system’s information network. “We know that if we add another barrier, they’re not going to use it,” Srini says. “We need to leverage the abilities they’ve already been trained in. It’s a very complex problem, but we’re hiding the complexity from them.”
—C. Vasko
Toward a Paperless Environment
Exploring Web-based document management
By Dana Hinesly
If you have seen one document management system, you have seen them all—right? Maybe not. The eLibrary Enterprise Suite from FileOn, Weston, Conn, takes a different approach to organizing the tons of paperwork flowing through hospitals each day.
“We are a software and services company, specializing in document management systems for health care enterprises,” says Anowar Shahjahan, president and CEO of FileOn. “Our specialty comes from integrating HL7 with registration and health information management systems [HIMS], providing anywhere access to review, analyze, code, and complete electronic patient records.”
FileOn’s solution combines an intelligent automation engine with barcode recognition software. To begin the process, paper files can be entered into the system from any scanning device, regardless of manufacturer. This intentional feature is designed to limit the amount of new hardware that hospitals must purchase to use the software.
“Many vendors give scanners to hospitals for free, because otherwise, they can’t sell their document solutions to them. But we decided not to build that part into the equation at all,” Shahjahan says, explaining how this frees up facilities to maintain existing documentation workflow. “We go in and look at a facility’s process, assisting with methodology and quality assurance, and then users can upload to the server from anywhere.”
Anyone with permission to log on to the system can do so from anywhere they can go online—whether it is an intranet, extranet, or Internet connection. Exactly who can gain access is governed through secure identification code.
Compatible with existing HIMS’, the eLibrary Enterprise Suite is a web-based software solution that, once installed, is virtually transparent to the users. Physicians, for example, log on to the hospital’s network as usual. Behind the scenes, the Suite routes the physician through the HL7 integration into the existing HIM.
“The solution logs them in automatically, taking them directly to that particular patient’s information,” Shahjahan says. “It also ensures that the information is secure: They can’t go anywhere else, except to that patient.”
When users search for a patient, the system produces a list of documents by date, each of which is converted into a secure hyperlink. When selected, this link connects them to the related information. Images are stored as TIFF files and are converted to PDF files so that they can be opened using the free Adobe software already installed on many computer systems.
“When scanned, most images take up only 50kbs to 150kbs; therefore, 5GB can store as much as 70,000 images,” Shahjahan explains. “For some customers, we have advised and provided NAS servers for as little as $3,000 with 500GB of Raid 5 storage, which is more than sufficient for most small to mid-sized customers.
“Additionally, upon agreement with customers, we often will get involved with the hardware sizing analysis and provide recommendations to the customer on the most cost-effective solutions in the market,” he continues. “Also, we often can implement the hardware setup, connect it to the network, and install all of our software remotely and support it remotely. As far as we can tell, there is no limit to how much we can scale this. It’s mostly dependent on the Windows operating system and Intel server performance.”
All of this technology and access is simple to navigate. Users likely will notice a strong resemblance between FileOn’s look and that of Microsoft’s Internet Explorer. The similarity is not coincidental. Because Explorer is one of the most commonly used browsers, FileOn patterned its user interface to mirror many of its qualities.
“Doctors and hospitals are busy, and the last thing you want them to do is take time away from their work to learn another interface,” Shahjahan notes. “Because the design for the patient information is very similar to Explorer, it further increases adoption because there’s nothing new to learn. We’ve been training new users in about a minute.”
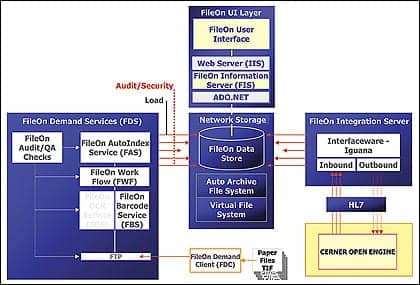 |
| Shown here is an illustration of how the FileOn solution has been implemented at Norwalk Hospital. The facility budgeted $23,000 for two production servers connected to SAN storage servers. |
Once in the system, documents—and the information they harbor—are available instantly and easily searchable. In addition to being able to execute effective queries, the program’s organization of the data lends itself to comprehensive, immediate corrections. If a patient name needs to be changed after the initial files have been entered into the system, for instance, the eLibrary Enterprise Suite makes easy work of what was once a labor-intensive, manual process. “As soon as the registration system is updated, it is immediately processed and updates every instance of that name; it goes all the way through every record in real time—seconds.”
FileOn sets itself apart in another way as well: The product costs less. To install and operate the entire solution, health care organizations should budget between $100,000 and $200,000. The exact amount varies based on the size of the hospital.
Teaming Up
The eLibrary Enterprise Suite for health care organizations is a result of a close collaboration between FileOn and the team at Norwalk Hospital, Fairfield County, Conn, where the FileOn solution was installed in September.
“We would not have been able to do this successfully without the participation of Norwalk Hospital’s staff. The quality assurance aspect of HL7 is so complex that without them, we would not have been able to be successful,” Shahjahan says. “These are patient records, so we worked with them to make sure the HL7 integration was so tight that there would be no chance of error.”
Marisa S. Barbieri, MS, is a senior software designer at Norwalk Hospital and founder of HospitalBarcoding.com; she was the project manager and the senior designer for the FileOn solution.
“[The FileOn software] was the backbone of an imaging tool,” she says. “Using barcoding as the main vehicle for document recognition, we customized it for use in our domain.”
Not only does the solution come complete with barcodes to identify 146 standard hospital forms, but FileOn’s Suite also is compatible with any existing custom forms or documents that a hospital may have in use. A standard registry kit allows facilities to create labels for forms that come in from outside health care agencies, such as those accompanying patients who are transferred to a hospital from one outside the system. Barcode labels can be adhered anywhere on the form.
The medical records team at Norwalk was the first to put the system to use, working exclusively on documents from the emergency department (ED) as quality analysis reviews are being performed to ensure the system’s performance. To date, Barbieri and her staff are very pleased. Eventually, staff in the ED will scan documents as the patient is processed.
 |
“Releasing this product to the point of care area is a very new concept in hospitals today, but we want to disseminate the information to our caregivers as fast as possible,” says Barbieri, who is a member of both the National Patient Safety Systems Committee of the Health Industry Business Communications Council (HIBCC) and the Bar Code Task Force of the Healthcare Information and Management Systems Society (HIMSS). “Barcodes have enabled us to do that, because if every document is encoded with [one], the document can identify itself and is electronically filed—as opposed to a manual intervention and review of the document with the human eye. And that is where you gain efficiencies.”
Because it is currently used only in the records room, the hospital has not conducted a form analysis of the exact savings—in both time and money—that have resulted from FileOn’s installation; however, anecdotal evidence indicates that the software has made a substantial impact already.
“Although I don’t have a quantitative number, the efficiencies have risen dramatically—it’s been amazing. In cases where it used to take days to get documents into the HIMS, it now takes minutes,” Barbieri notes. “We’ve seen efficiencies in the medical records department: Before they had to manually intervene on every single document and index it, and now, they just scan it and it goes into the folder of the right patient.”
Number-crunching aside, Norwalk Hospital has noted the impact that the solution has made on patient care—and the improved workflow and throughput that are a direct result of the solution.
“We want to make sure that the physicians have the most up-to-date information on the patient, and FileOn’s solution disseminates the information days earlier than what we’re used to,” Barbieri says. “It improves patient care, and that’s our bottom line here at Norwalk.”
Dana Hinesly is a contributing writer for Axis Imaging News. For more information, contact .
Alliance Aims to Transform Data Into Actionable Information
GE Healthcare Inc, Waukesha, Wis, has announced its strategic alliance with DataMasters Inc, Wyomissing, Pa, to leverage the power of DataMasters’ Precision.BI (Business Intelligence) product for GE Healthcare’s new Centricity suite of business solutions. Specifically, the DataMasters product will collect complex organizational data and processes and translate the data into result-oriented information for health care professionals. This will enhance the performance of GE’s Centricity Business revenue cycle management solution.
“Our customers are demonstrating the desire and readiness to push analytical and reporting capabilities further into their end-user base, including managers, business staff, clinicians, and executives,” Jeff Kao, vice president and general manager of integrated IT solutions at GE Healthcare, said in a press release. “This partnership combines the proven data model and usability of Precision.BI with the business expertise of GE Healthcare to create a solution designed to transform business data into intelligent and actionable information.”
The combined solution, called Centricity Business–Informatics, can be deployed rapidly to help health care organizations apply enhanced business intelligence capabilities. Key performance indicators and Dashboard subject areas include AR Aging and Balances, AR Trends, Provider Utilization, Collection Analysis, Income Analysis, Service Analysis, Scheduling, and other critical management metrics.
Visit www.gehealthcare.com or www.precisionbi.com for additional information.
